
Downloaded 611 times
![DRUGS FOR BRONCHIAL ASTHMA
EDITED BY:
PRITHWIRAJ MAITI, MBBS
HOUSE PHYSICIAN
DEPARTMENT OF INTERNAL MEDICINE, R.G.KAR MEDICAL COLLEGE
AUTHOR: “AN ULTIMATE GUIDE TO COMMUNITY MEDICINE”
AUTHOR: “A PRACTICAL HANDBOOK OF PATHOLOGY SPECIMENS AND SLIDES”
[BOTH PUBLISHED BY JAYPEE BROTHERS MEDICAL PUBLISHERS, INDIA]](https://image.slidesharecdn.com/drugsforbronchialasthma-160922133453/75/Drugs-for-Bronchial-Asthma-1-2048.jpg)








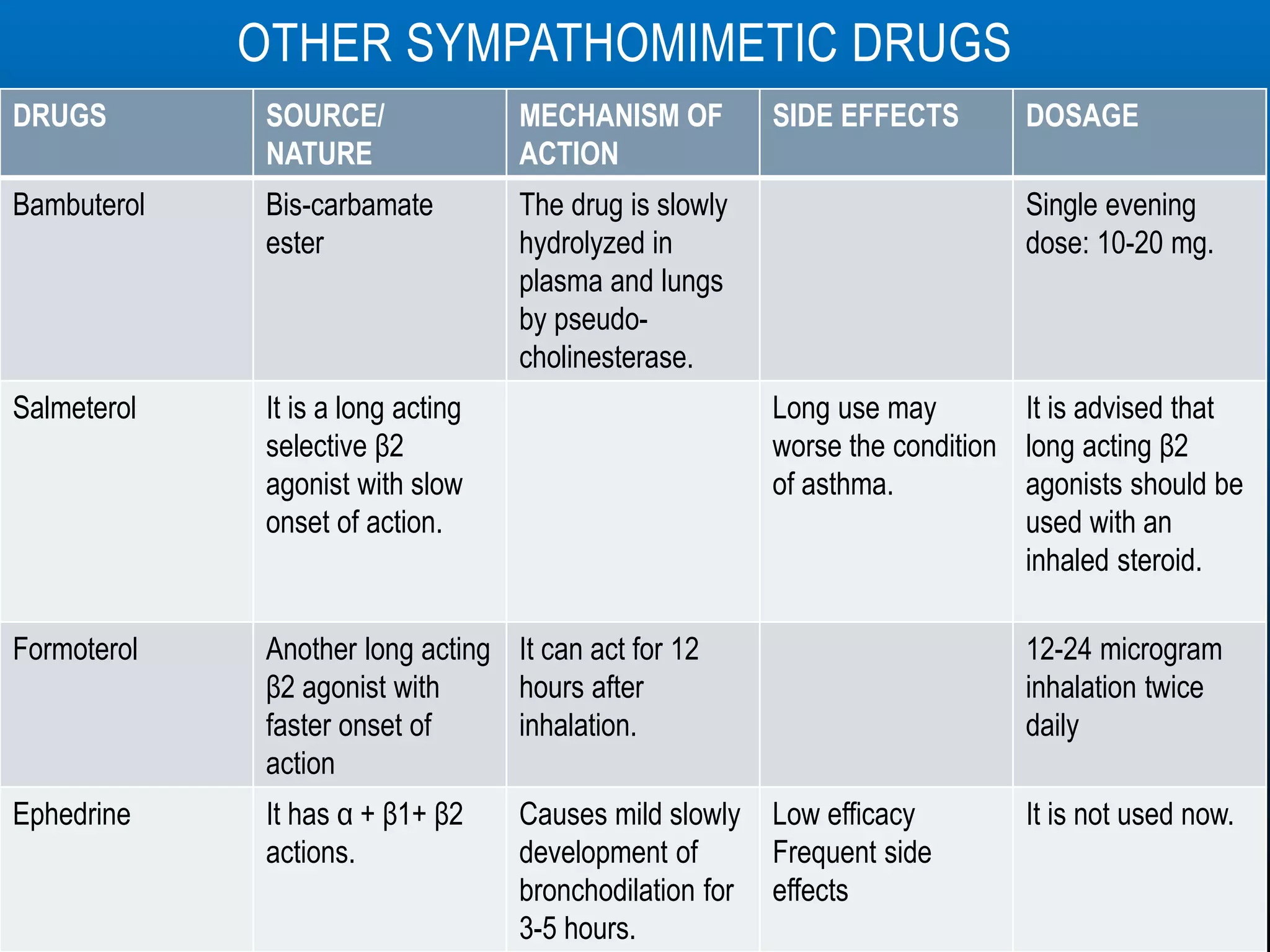







































The document provides an extensive overview of bronchial asthma, including its definition, symptoms, types, mechanisms, and treatment approaches. It details various drug classifications used in treatment such as bronchodilators, corticosteroids, leukotriene antagonists, and mast cell stabilizers, while discussing their mechanisms of action, uses, and potential side effects. Key medications like salbutamol, theophylline, and others are illustrated with their pharmacokinetics, dosages, and interactions.





































































































