Downloaded 1,139 times












![TREATMENT (ACQUIRED AND
HEREDITARY HYPOPARATHYROIDISM)
1. Vitamin D [40,000-120,000 U/d] or
1,25(OH)2*D3*(calcitriol) [0.5-
1microgm/day] ?
2. High oral calcium intake.
3. Thiazide diuretics?
(Hydrochlorothizide 12.5-50mg)](https://image.slidesharecdn.com/hypocalcemia-130217123548-phpapp02/75/Hypocalcemia-16-2048.jpg)















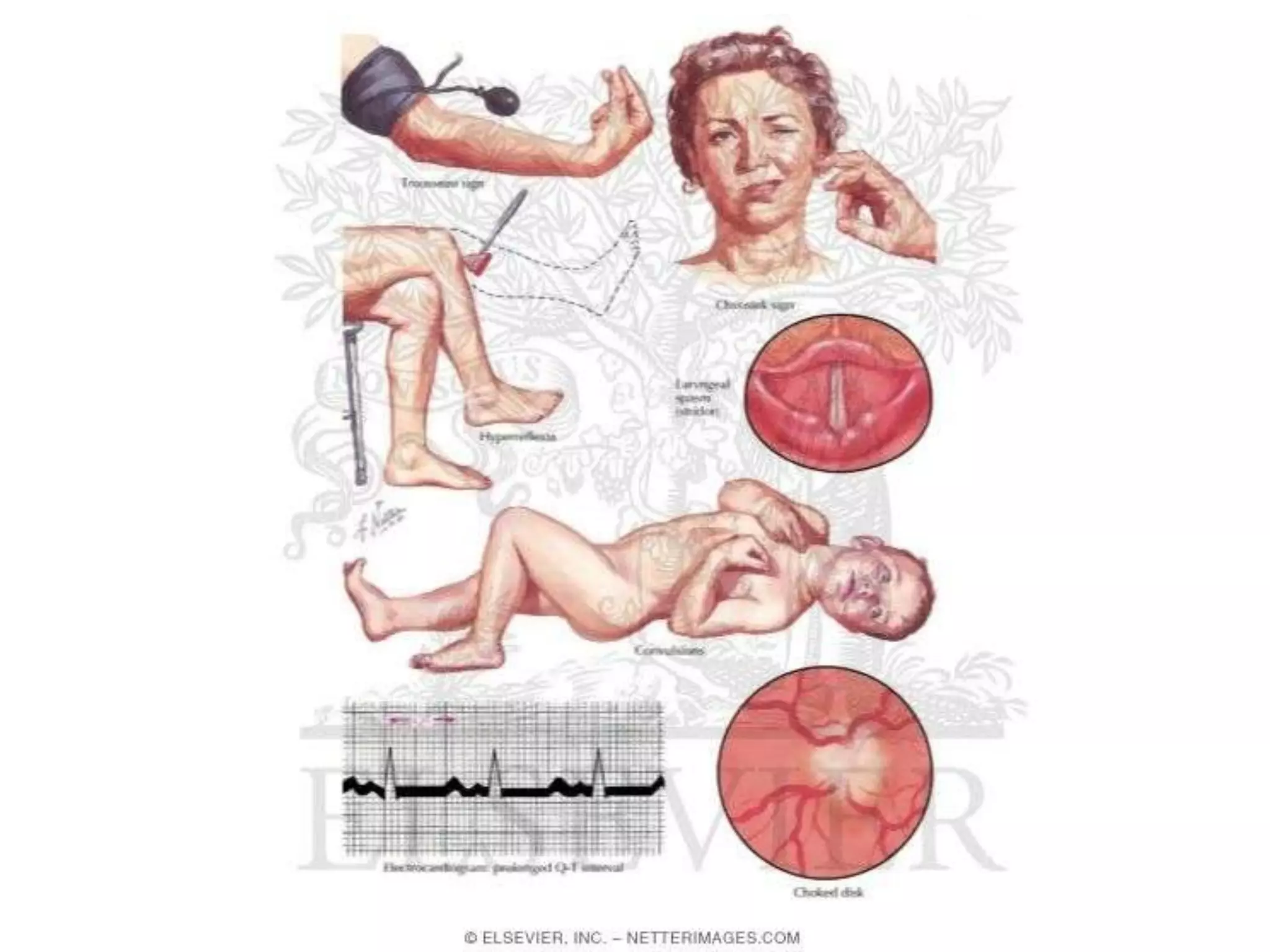
This document discusses hypocalcemia, defined as a serum calcium level below 8.5 mg/dl. It may be caused by low or high parathyroid hormone levels. Causes of low PTH include parathyroid gland agenesis, destruction, or dysfunction. Causes of high PTH include vitamin D deficiency, kidney disease impairing vitamin D activation, or drugs. Symptoms include increased neuromuscular excitability. Investigations include calcium, albumin, phosphorus, magnesium and PTH levels. Treatment involves vitamin D, calcium supplements, and magnesium as needed.






























































