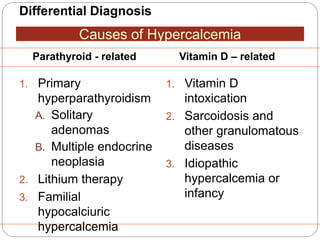
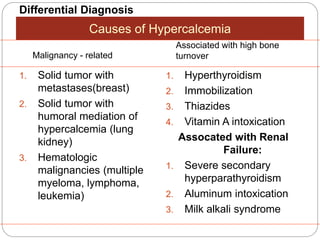
The document outlines disorders related to the parathyroid glands, focusing on the regulation of calcium, phosphate, and magnesium homeostasis by parathyroid hormone (PTH) and calcitonin. It discusses conditions such as primary and secondary hyperparathyroidism, their causes, clinical features, and diagnosis, alongside treatment options including surgical intervention. Additionally, it reviews hypoparathyroidism and pseudohypoparathyroidism, emphasizing the biochemical and clinical implications of these disorders.




























































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

