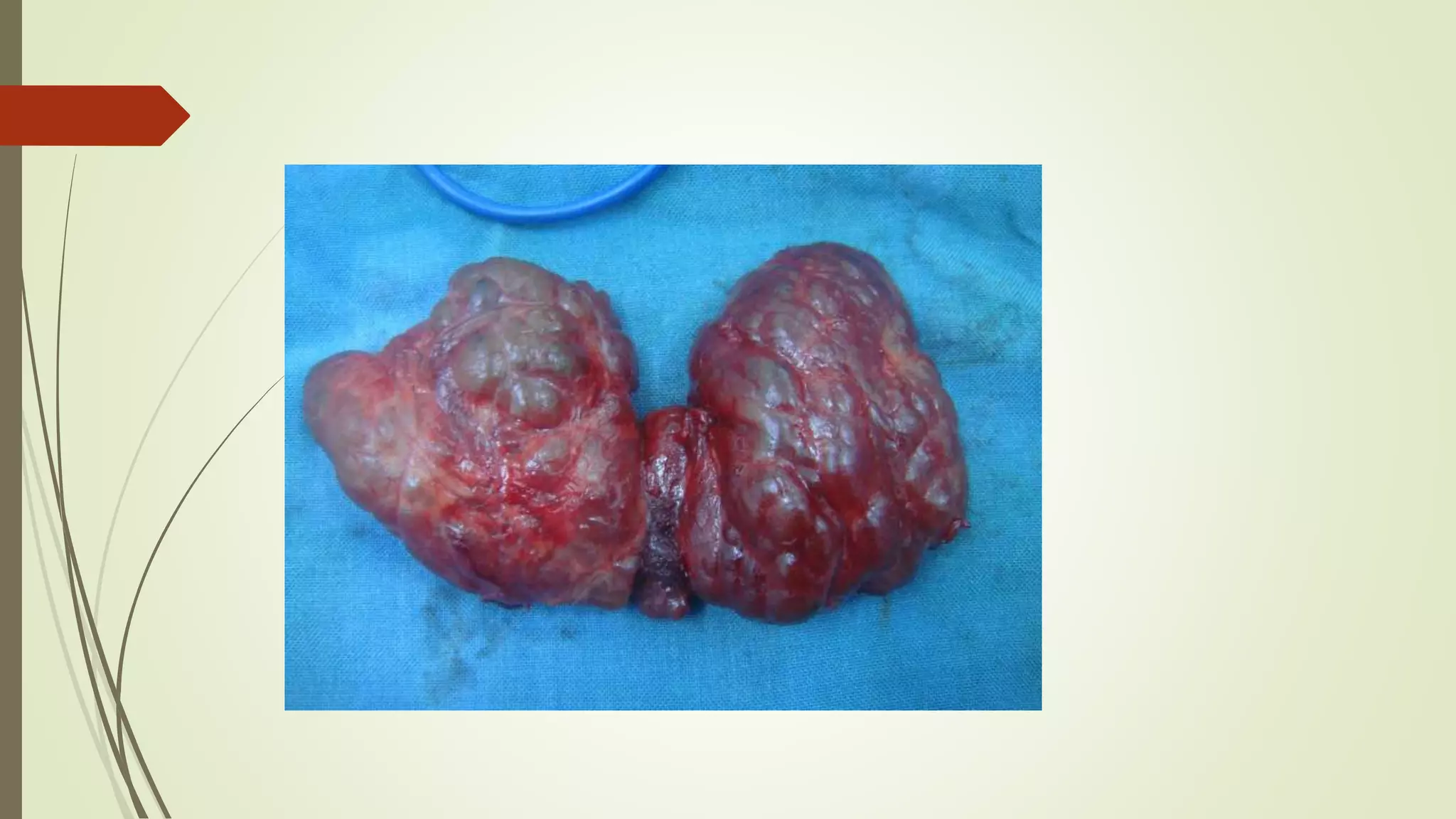
Multinodular goitre (MNG) is characterized by the growth of multiple nodules within the thyroid gland that are structurally and functionally altered. It develops through stages of thyroid hyperplasia and hypertrophy followed by fluctuations in TSH levels which promote the formation of inactive nodules within areas of active and inactive thyroid tissue. MNG most commonly affects middle-aged females and presents as a slowly progressive disease with multiple, firm nodules of varying sizes within the thyroid gland. While often benign, MNG can potentially lead to complications such as hyperthyroidism, thyroid cancer, or tracheal obstruction.















































![THYROID_GLAND[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/thyroidgland1-231005071359-bdb08841-thumbnail.jpg?width=640&height=640&fit=bounds)


























