Downloaded 414 times
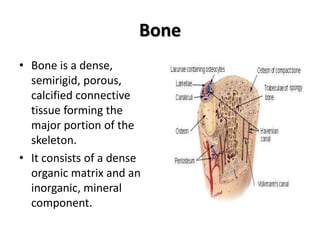
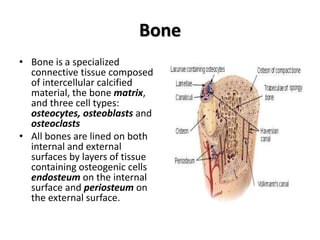
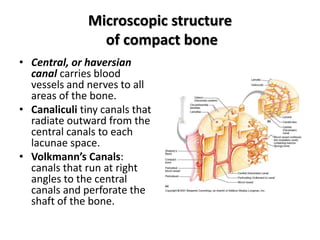
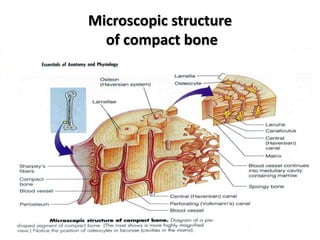
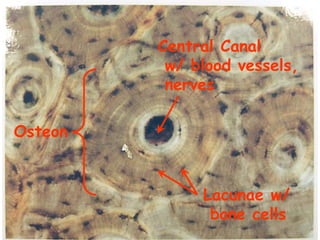
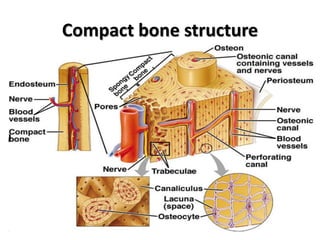
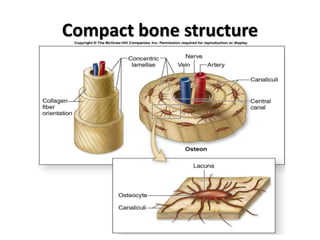
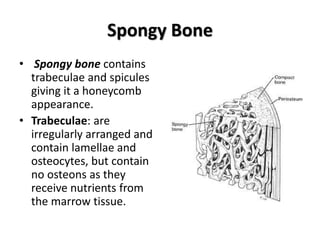
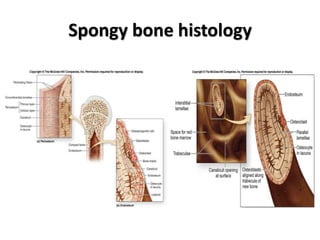
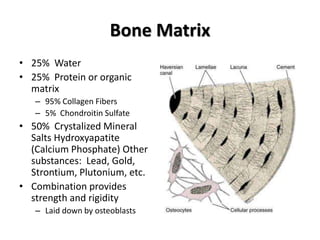
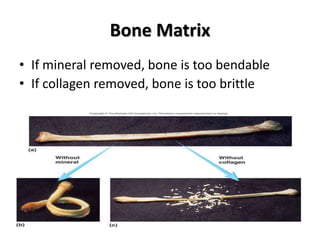
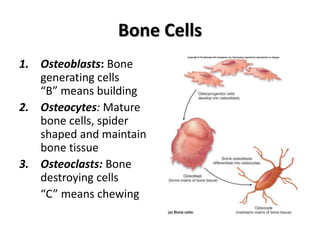
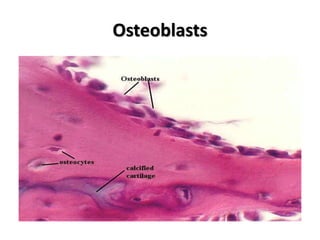
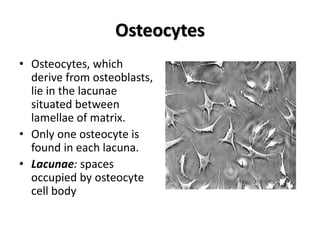
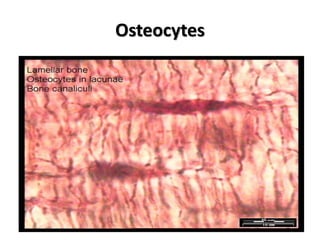
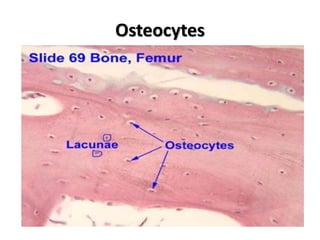
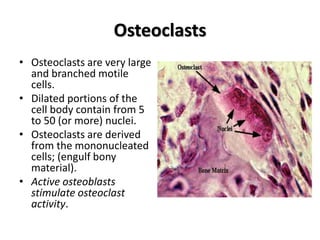
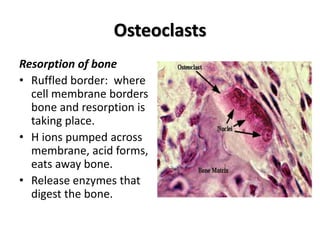
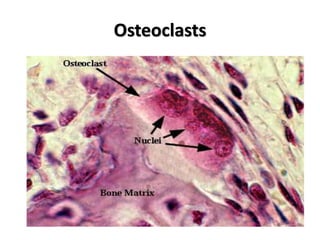
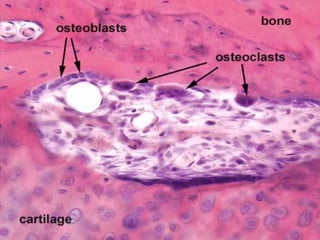
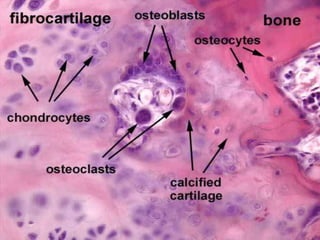
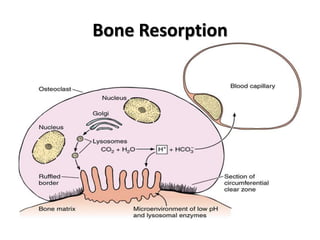
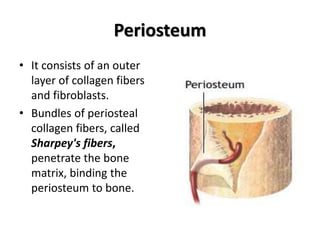
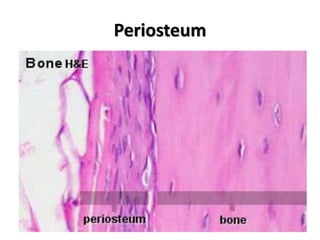
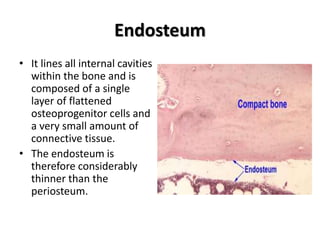
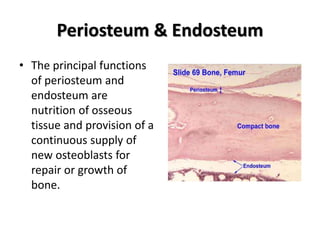
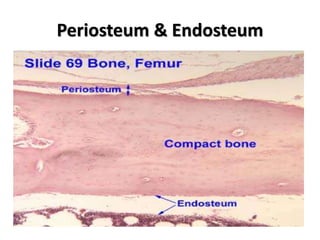


This document provides an overview of bone histology. It defines bone as a mineralized connective tissue composed of bone matrix and three cell types: osteoblasts, osteocytes, and osteoclasts. It describes the microscopic structure of compact and spongy bone, including osteons, central canals, lamellae, and trabeculae. It explains the functions of osteoblasts in bone formation, osteoclasts in bone resorption, and osteocytes in bone maintenance. Finally, it discusses the periosteum and endosteum, which cover the external and internal bone surfaces and provide nutrition and new osteoblasts.





























































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)

![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)











