Downloaded 251 times

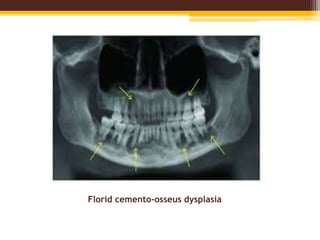

This document discusses fibrous dysplasia and cemento-osseous dysplasia, two fibro-osseous lesions of bone. It covers the classification, etiology, clinical features, radiographic appearance, histopathology, and treatment of these conditions. Specifically, it describes how fibrous dysplasia is caused by a mutation leading to overproduction of cAMP, and can present as monostotic or polyostotic lesions. It also outlines the three types of cemento-osseous dysplasia - focal, periapical, and florid - based on clinical and radiographic characteristics.































































































