Downloaded 46 times
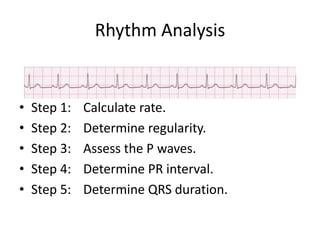
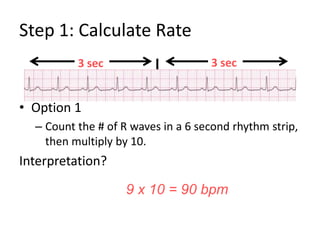
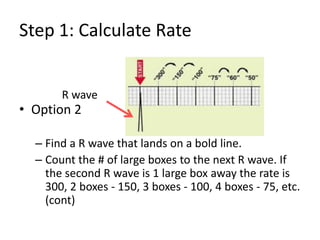
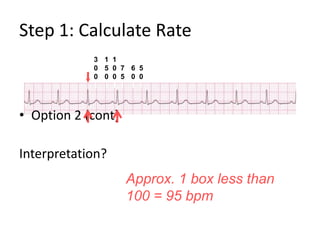
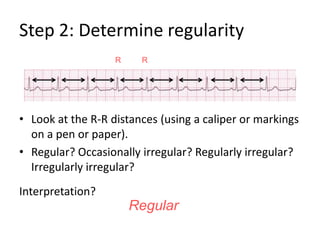
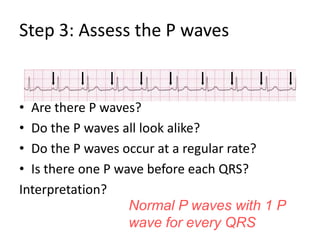
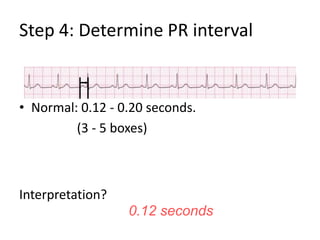
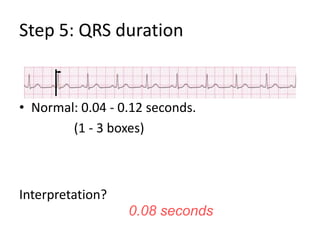
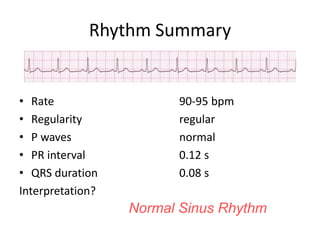
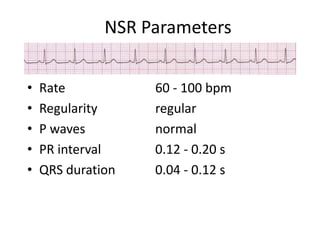
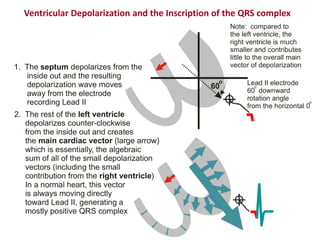
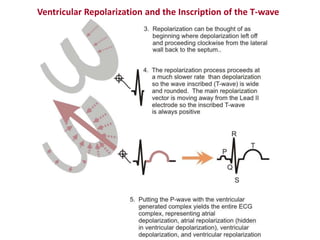
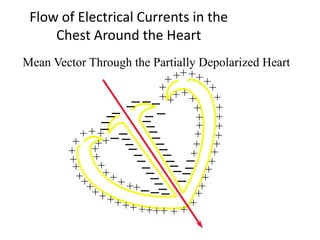
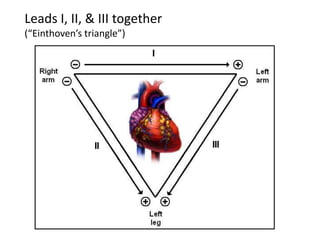
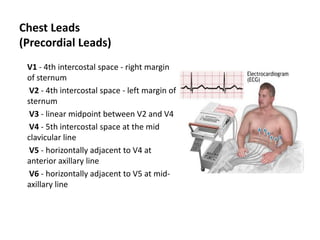

This document provides instructions for analyzing cardiac rhythms based on an electrocardiogram (ECG). It describes 5 steps: 1) calculating the heart rate, 2) determining rhythm regularity, 3) assessing P waves, 4) measuring the PR interval, and 5) measuring QRS duration. Normal values for these metrics in normal sinus rhythm are also provided. The document additionally covers ECG lead placements and how the cardiac electrical conduction system generates the ECG tracings.
































![Shadechapter03.ppt [read only]](https://cdn.slidesharecdn.com/ss_thumbnails/shadechapter03-150421101919-conversion-gate02-thumbnail.jpg?width=640&height=640&fit=bounds)

















































