![COMPOSITION OF BONE
- BONE SALTS
• Crystalline salts present in bones are called
Hydroxyapatites [Ca10(PO4)6(OH)2], which contains
calcium and phosphate.
• Others salts are also present.
• Strengthen the bone matrix.
11
Oral Histology (Development, Structure &
Function) A.R.Ten Cate, 5th & 6th edition](https://image.slidesharecdn.com/1gds6w1atkgxpax55m5n-signature-11bfc635dadd10a3a09f0305d36d2634b5c4d35ec2e6d3761fabe8171afe7f12-poli-160505064926/85/Bone-Its-Importance-to-Prosthodontist-11-320.jpg)
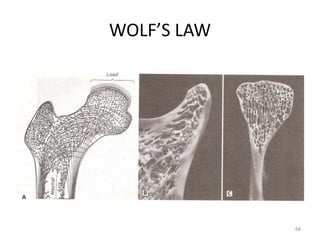
![WOLF’S LAW
• Wolff’s Law [Julius Wolff, German anatomist,
1836-1902]
• “For a uniform or constant fact or principle,
more specifically, that a bone, either normal
or abnormal, will develop the structure most
suited to resist those forces acting on it.”
GPT, 8TH EDITION
67](https://image.slidesharecdn.com/1gds6w1atkgxpax55m5n-signature-11bfc635dadd10a3a09f0305d36d2634b5c4d35ec2e6d3761fabe8171afe7f12-poli-160505064926/85/Bone-Its-Importance-to-Prosthodontist-67-320.jpg)

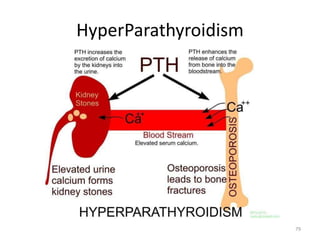
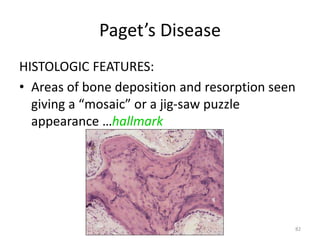

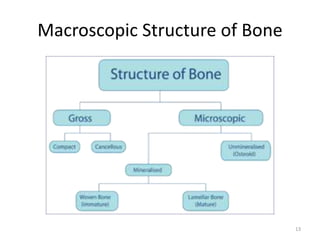
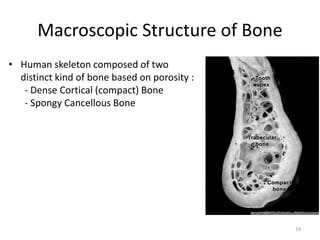
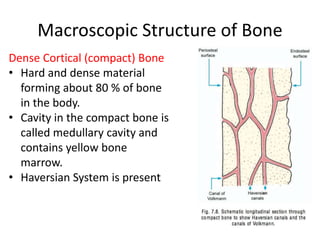
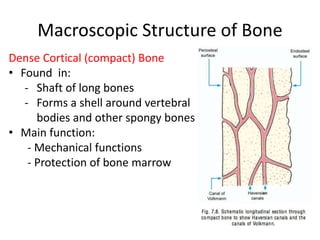
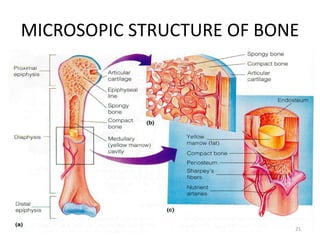
Bone is a hard connective tissue that forms the skeleton. It has an inorganic mineral component made up of calcium salts and an organic collagen matrix. Bone comes in two types - dense cortical bone forming the hard outer shell and spongy cancellous bone on the inside. Bone is constantly remodeled through the actions of bone-forming osteoblasts and bone-resorbing osteoclasts. Diseases like osteoporosis weaken the bones through decreased bone density while Paget's disease involves abnormal bone deposition and resorption.








![Recent advancements in denture base materials [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/recentadvancementsindenturebasematerialsautosaved-181219143003-thumbnail.jpg?width=640&height=640&fit=bounds)