Downloaded 353 times

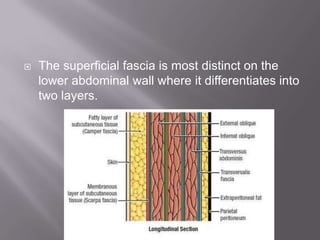
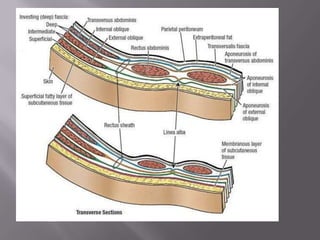
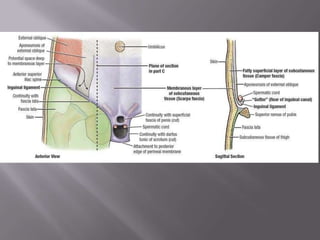

The document summarizes the anatomy and characteristics of fascia. It describes the superficial fascia as a layer of loose connective tissue that connects the skin to underlying structures, with variable thickness, fat content, and presence of flat sheets of muscle in some regions. The quantity of subcutaneous fat differs between sexes and climates. The superficial fascia is most distinct on the lower abdominal wall, differentiating into two layers. It is also well differentiated in the limbs, perineum, and thin in other areas. Deep fascia forms a membrane wrapping the limbs and body wall with varying thickness and absence in some areas. It is firmly anchored to underlying bone and surrounds neurovascular structures in the neck.





























































![Integumentary system[1]](https://cdn.slidesharecdn.com/ss_thumbnails/et4ixbnntvemxpiiz5zf-signature-460517c25b85fc4e63c8080c3e27df73c8dfae9e0c6544cc7ea6d9e8b5e79cc7-poli-180213064029-thumbnail.jpg?width=640&height=640&fit=bounds)













































