Downloaded 383 times
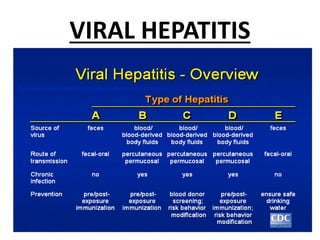
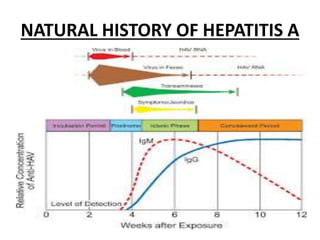

This document provides information about Hepatitis A virus (HAV) and Hepatitis A disease. It states that HAV is the causative agent of Hepatitis A, an acute infectious disease. The virus is transmitted primarily through the fecal-oral route. Symptoms include fever, jaundice, and fatigue. While the disease is usually self-limiting, vaccination and improved sanitation can help prevent transmission.