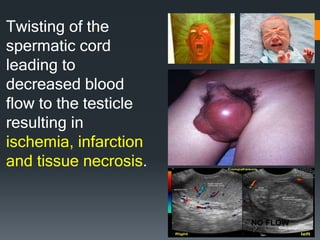
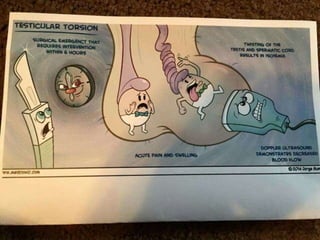
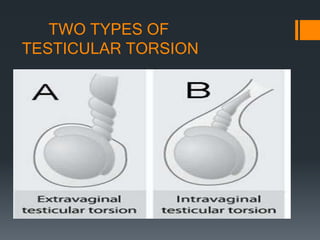
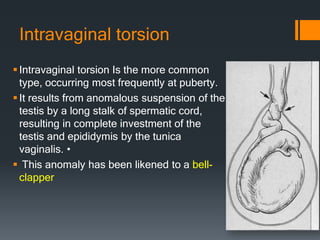
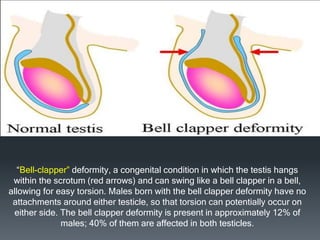
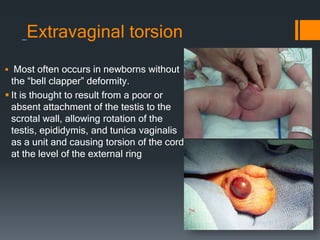
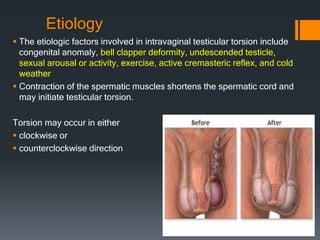
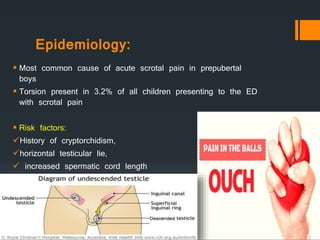
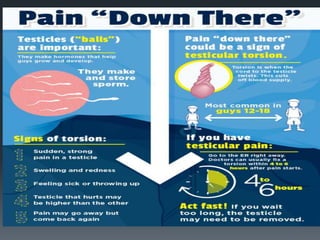
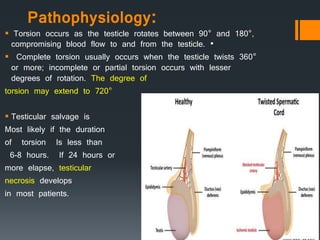

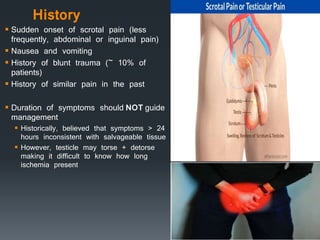
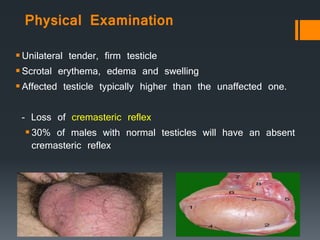
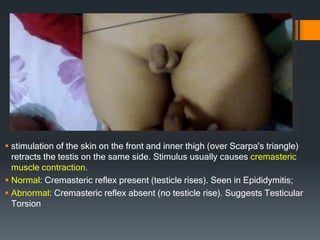



Testicular torsion occurs when the spermatic cord twists, reducing blood flow to the testicle. There are two main types - intravaginal torsion which is more common and often seen at puberty due to a "bell-clapper" deformity, and extravaginal torsion which occurs in newborns without this deformity. Risk factors include a history of cryptorchidism or an abnormally long spermatic cord. Physical exam may reveal an elevated, tender testicle with absent cremasteric reflex. Ultrasound can show reduced blood flow, but surgery should not be delayed for imaging. Manual detorsion can be attempted in some cases but all patients require surgical exploration to detorse