Downloaded 1,759 times
![Hematuria
The presence of blood/RBCs in the
urine
Dr. Prajwal Ghimire
Origin:[hemato- [G. haima (haimat-)]+ G. ouron, urine]](https://image.slidesharecdn.com/hematuriamedicalpost-121108115831-phpapp01/85/Hematuria-1-320.jpg)
![Hematuria
The presence of blood/RBCs in the
urine
Dr. Prajwal Ghimire
Origin:[hemato- [G. haima (haimat-)]+ G. ouron, urine]](https://image.slidesharecdn.com/hematuriamedicalpost-121108115831-phpapp01/75/Hematuria-1-2048.jpg)
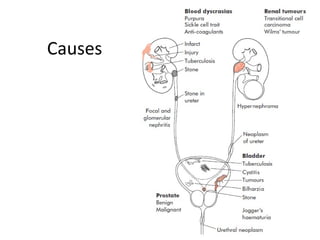


Hematuria is defined as the presence of blood or red blood cells in the urine. It can be macroscopic (visible to the naked eye) or microscopic. Common causes include urinary tract infections, kidney diseases, cancers, and stones. A urinalysis and urine culture can help identify infection, while imaging tests like ultrasound, CT, and cystoscopy can locate any abnormalities in the kidneys, ureters, bladder, or urethra. Further blood tests may also indicate underlying conditions. Hematuria is investigated through examination of urine and imaging of the urinary tract to diagnose the cause.




















































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)














