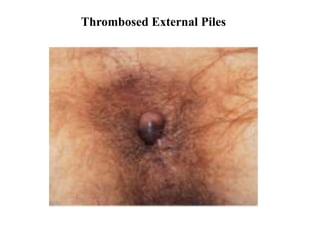
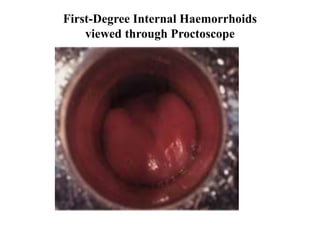
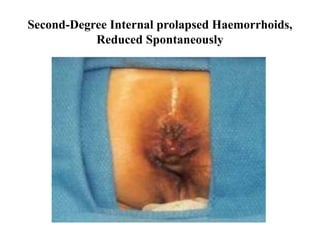
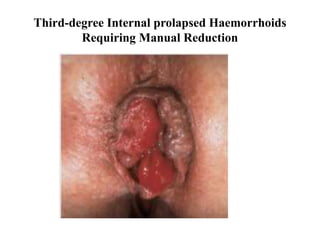
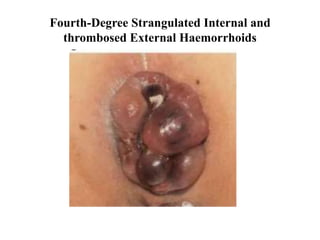
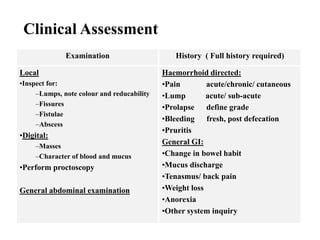
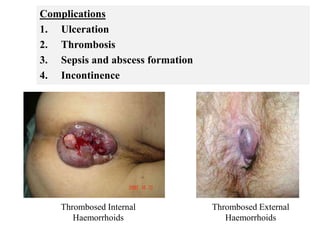
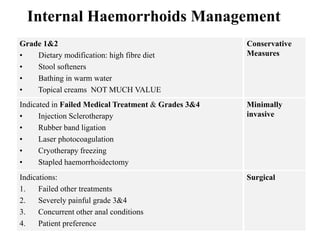
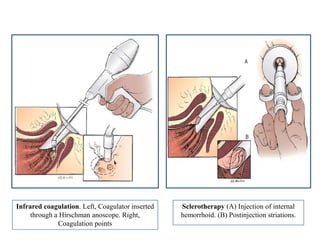
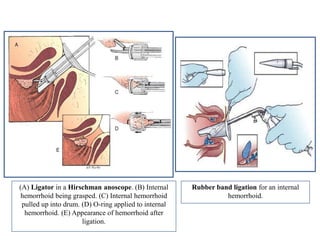
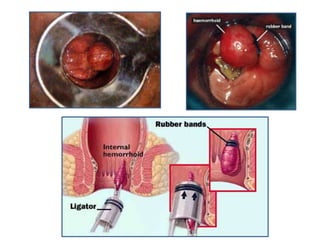
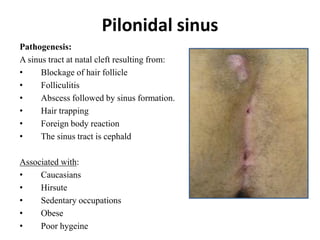
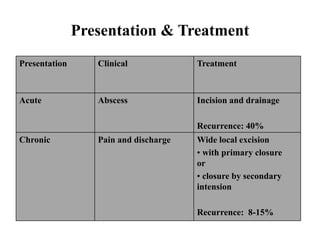
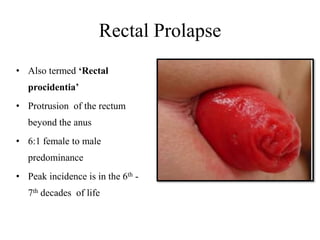
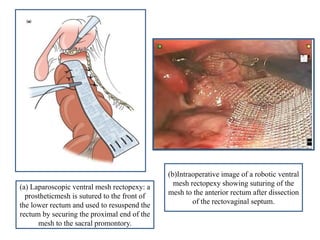
The document provides detailed information on various anorectal disorders, including their anatomy, definitions, pathogenesis, clinical features, diagnostic methods, and management strategies for conditions such as hemorrhoids, anal fissures, pilonidal sinus, perianal abscess, and fistula in ano. It describes the risk factors, classification, and specific treatments for each condition, highlighting the importance of clinical assessment and tailored management plans. Various conservative and surgical interventions for different grades of hemorrhoids and anal fissures are emphasized, along with potential complications associated with these disorders.