









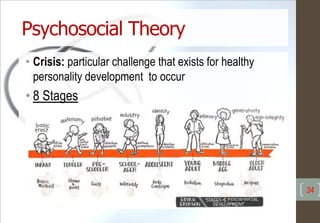
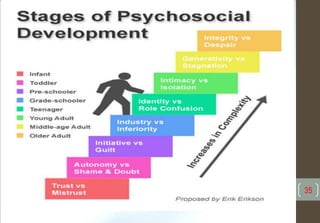
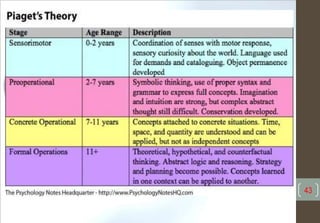
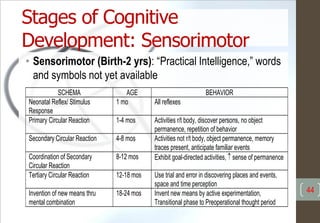
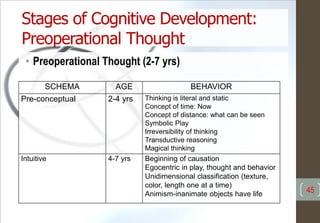
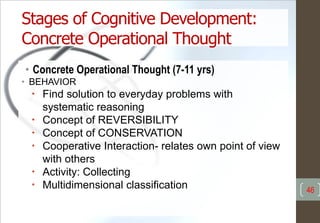
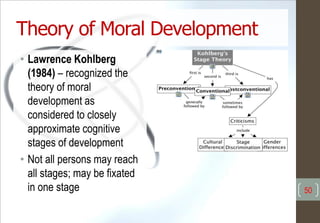
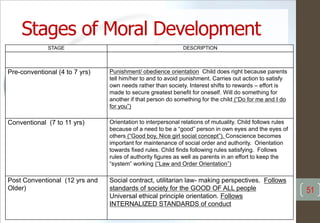
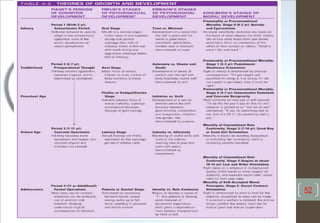









Growth and development principles, theories, and concepts are essential for nursing care of children. Principles include growth occurring at different rates in different parts of the body. Major theories discussed are Freud's psychosexual theory focusing on psychosexual development, Erikson's psychosocial theory addressing psychosocial tasks, Piaget's cognitive development theory outlining stages of cognitive growth, and Kohlberg's moral development theory. Nursing interventions should be based on understanding of children's developmental needs and abilities at different ages and stages.





















































![Growth & Devt[1].](https://cdn.slidesharecdn.com/ss_thumbnails/growth-devt1-1215090495508239-9-thumbnail.jpg?width=640&height=640&fit=bounds)




















































