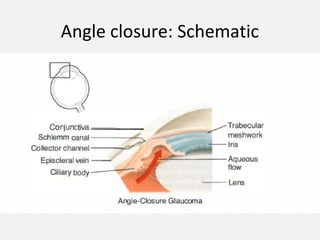
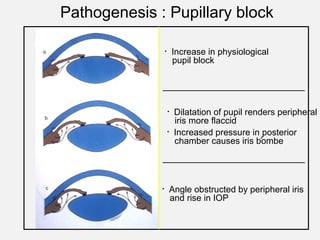
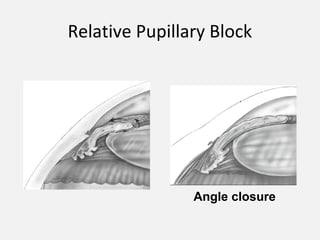
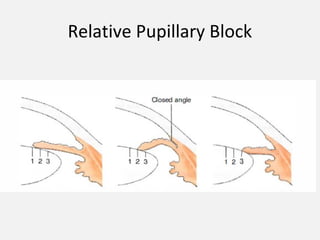
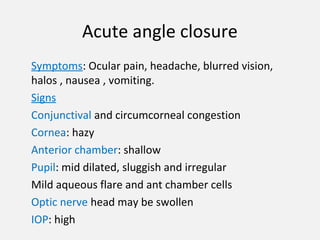
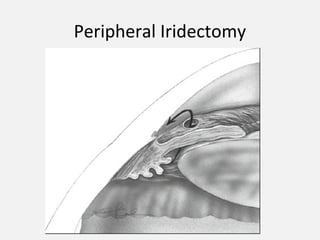
Angle-closure glaucoma is caused by apposition of the peripheral iris to the trabecular meshwork, reducing drainage of aqueous humor from the eye. Primary angle-closure glaucoma (PACG) has no underlying cause and is due to anatomic factors. It is a leading cause of glaucoma worldwide. PACG presents with acute symptoms like eye pain and blurred vision due to sudden rise in pressure from pupillary block. Treatment involves lowering pressure with medications or iridectomy to prevent future attacks. Long-term management focuses on screening and treatment to prevent angle closure in the fellow eye.