
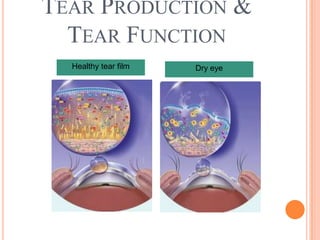
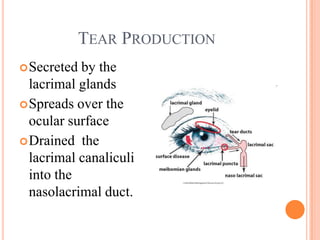
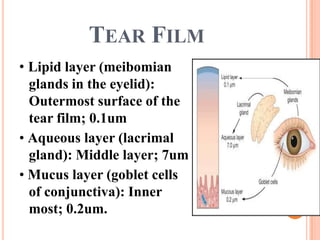

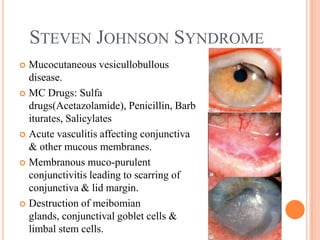
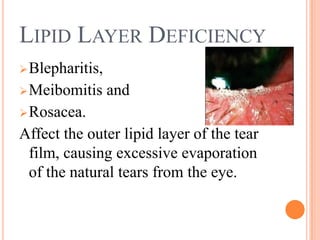
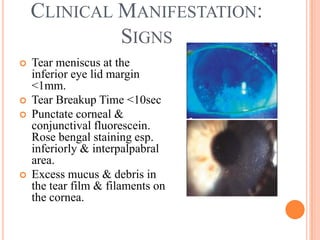
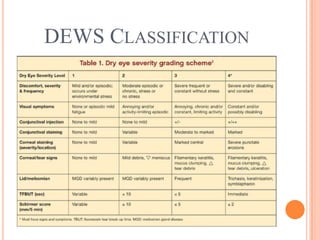

Dry eye occurs when there is inadequate tear production or function, resulting in an unstable tear film and ocular surface disorder. It can be caused by conditions that reduce tear production such as Sjogren's syndrome, vitamin A deficiency, Stevens-Johnson syndrome, or medications. Other causes affect the tear film layers, like meibomian gland dysfunction reducing the outer lipid layer. Symptoms include dryness, burning, and blurred vision. Treatment focuses on replacing tears, improving ocular surface health, addressing underlying causes, and escalating care based on severity through the DEWS treatment guidelines.

























































![Dry_Eye_Presentation_Final[1].pptx......](https://cdn.slidesharecdn.com/ss_thumbnails/dryeyepresentationfinal1-250516163834-f963ff70-thumbnail.jpg?width=640&height=640&fit=bounds)

























