



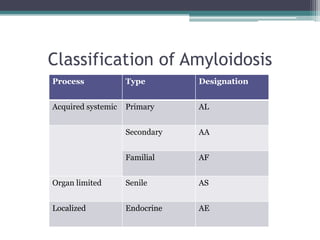















































This document provides information on amyloid, including: - Amyloid is an abnormal protein structure characterized by beta-pleated sheet conformation that takes up Congo red dye and exhibits green birefringence under polarized light. - The main components of amyloid deposits are fibril proteins that make up 85-90% and the P component that stabilizes fibrils and decreases clearance. - Amyloidosis is classified by process (acquired vs hereditary), type (AL, AA, AF etc), and location (systemic vs localized). Important systemic forms involve immunoglobulin light chains, serum amyloid A, and transthyretin. - Amyloid is demonstrated histologically using stains








































































































