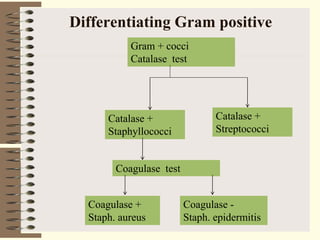
Gram positive bacteria include cocci like Staphylococcus and Streptococcus, as well as rods like Bacillus. Major pathogens in the genus Staphylococcus include Staphylococcus aureus and coagulase-negative staphylococci like S. epidermidis. S. aureus is a major human pathogen capable of causing skin infections like boils and abscesses, as well as toxin-mediated diseases like food poisoning and toxic shock syndrome due to virulence factors like coagulase and various toxins. Coagulase-negative staphylococci are generally opportunistic pathogens of immunocompromised individuals.




































































![Staphylococcus_lecture. FUHSA 2025 [Compatibility Mode].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/staphylococcuslecture-250716105746-0d9f38b5-thumbnail.jpg?width=640&height=640&fit=bounds)




















