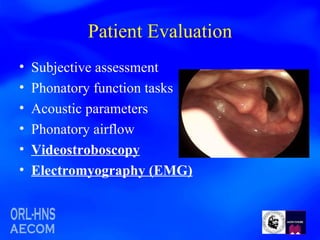
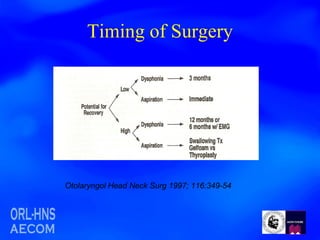
1. Videostroboscopy and laryngeal electromyography (EMG) can be used to determine the etiology of an immobile vocal fold in a patient with hoarseness after aortic aneurysm repair.
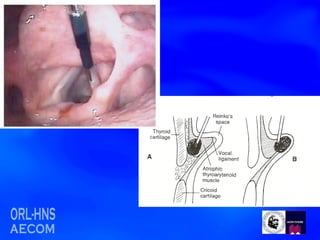
2. The difference between vocal fold medialization injection and intrachordal injection is that medialization injects material lateral to the vocalis muscle while intrachordal injection injects material just deep to the lamina propria to eliminate soft tissue defects.
3. Materials available for unilateral vocal fold medialization by injection include Teflon, human micronized alloderm, autologous fat, gelfoam, collagen, and hyaluronic acid formulations; alloderm
















































































![784cdysphonia[1]](https://cdn.slidesharecdn.com/ss_thumbnails/784cdysphonia1-1234158878157310-2-thumbnail.jpg?width=640&height=640&fit=bounds)



























