The document summarizes the National Ambulatory Medical Care Survey (NAMCS) and the National Hospital Ambulatory Medical Care Survey (NHAMCS), which collect data on outpatient visits through annual probability samples. Key points include:
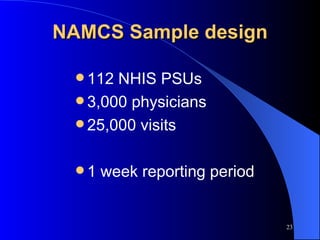
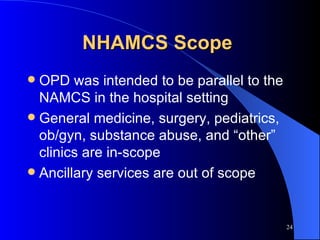
1) NAMCS collects data from office-based physicians while NHAMCS collects data from emergency and outpatient departments.
2) The surveys were established in the 1970s and track health care practices, conditions, priorities, and Healthy People objectives.
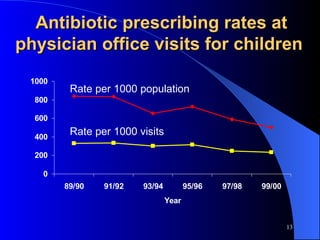
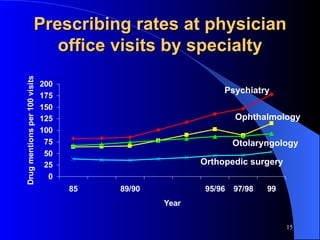
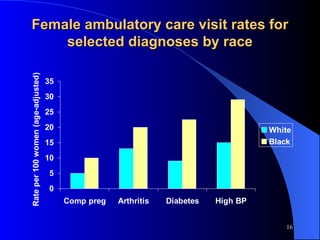
3) Data is used by medical groups, government agencies, researchers and media to inform policy, study prescribing rates, and more.



![I need more information ! Visit the Research Data Center booth E-mail: [email_address] Website: www.cdc.gov/nchs/r&d/rdc.htm Call (301) 458-4277](https://image.slidesharecdn.com/mccaigwoodwell2-1234160274069708-1/85/Mccaig-Woodwell2-78-320.jpg)
![Thank You Linda McCaig – NHAMCS data [email_address] David Woodwell – NAMCS data [email_address]](https://image.slidesharecdn.com/mccaigwoodwell2-1234160274069708-1/85/Mccaig-Woodwell2-79-320.jpg)
































































![784cdysphonia[1]](https://cdn.slidesharecdn.com/ss_thumbnails/784cdysphonia1-1234158878157310-2-thumbnail.jpg?width=640&height=640&fit=bounds)






























