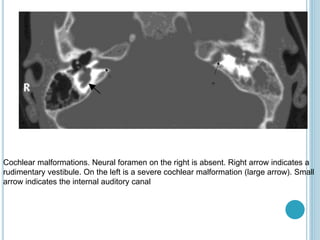
Cochlear implants can help those with severe to profound hearing loss by making speech a viable communication option. They improve speech perception, production, and reading outcomes. Candidates undergo testing to determine candidacy and benefit from a hearing aid trial first. Imaging is needed to assess anatomy and rule out contraindications like 8th nerve lesions. Successful implantation requires a collaborative team approach and post-operative rehabilitation. Risks include wound issues, facial nerve stimulation, and device problems.











































![cochlear implant [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cochlearimplantautosaved-230807191245-e9fc2957-thumbnail.jpg?width=640&height=640&fit=bounds)




![Recent_Advances_Cochlear_Implant_Candidacy_Dr_Anand_Gupta[1]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/recentadvancescochlearimplantcandidacydranandgupta1-1-251128040227-e519dadb-thumbnail.jpg?width=640&height=640&fit=bounds)



































