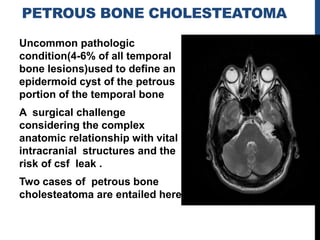
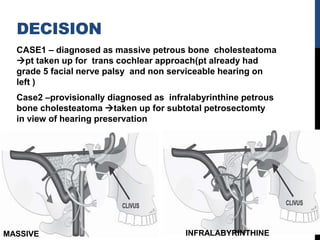
This document discusses two cases of petrous bone cholesteatoma. It provides background on petrous bone anatomy and classifications of petrous bone cholesteatoma. It also describes the surgical approaches and considerations for treatment of petrous bone cholesteatoma, which aim to completely remove the disease while preserving vital structures like the facial nerve. Two cases of petrous bone cholesteatoma are presented and the surgical treatments used in each case.



![PBC-CLASSIFICATION
According to Sanna et al. [1993] PBCs can be classified into
five groups:
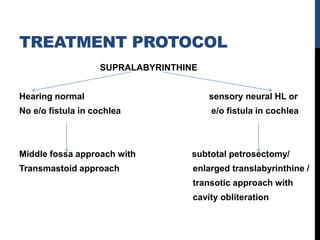
supralabyrinthine-geniculate ganglion
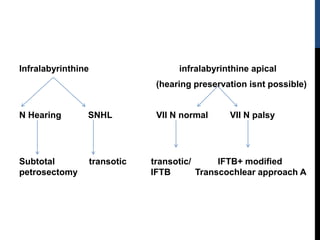
infralabyrinthine-hypotympanic and infralabyrinthine cells
infralabyrinthine-apical-infralabyrinthine compartment
extending to petrous apex
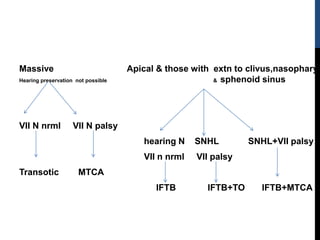
Massive-otic capsule
Apical-petrous apex
These terms describe both the location and the extent of the
lesion.](https://image.slidesharecdn.com/petrouscholesteatomasample-180207102625/85/Petrous-cholesteatoma-sample-14-320.jpg)
![1.Subaarcuate
via arch of scc-FRECKNER
2.Retrolabyrinthine
Superior to lscc & posterior to superior
scc-THORNWALDT
3.Infralabyrinthine(hearing preserving)
inferior to posterior scc
posterior to VII nerve and superior to
jugular bulb[DEARMIN &FARRIOR]
4.Subcochlear/infracochlear-(hearing
preserving)hypotympanic air cell tract
between ica,jugular bulb and
cochlea[FARRIOR]
5/6.peritubal–
b/w ica,cochlea and tegmen
5-Ramdier/lempert
6-Kopetsky/Almoor
7.Middle cranial fossa (hearing
preserving) EAGLETON](https://image.slidesharecdn.com/petrouscholesteatomasample-180207102625/85/Petrous-cholesteatoma-sample-16-320.jpg)