Downloaded 100 times
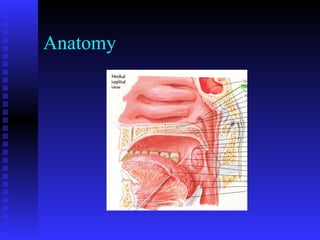
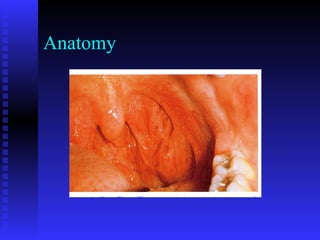
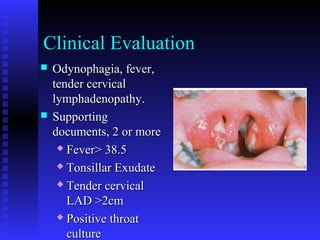





This document discusses tonsillitis, tonsillectomy, and adenoidectomy. It provides details on: - The history and anatomy of these procedures - Clinical evaluation and differential diagnosis of tonsillitis - Surgical indications and techniques for tonsillectomy and adenoidectomy - Preoperative evaluation and management of bleeding disorders - Adjuvant therapies like antibiotics, steroids, and local anesthetics to improve postoperative outcomes











































![Nasal septum and its diseases[1]](https://cdn.slidesharecdn.com/ss_thumbnails/nasalseptumanditsdiseases1-140421073429-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)











































