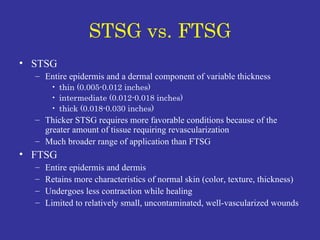
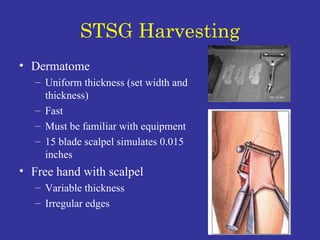
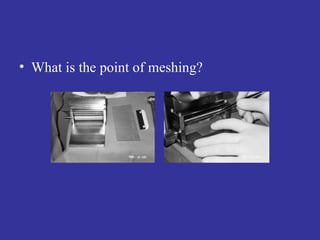
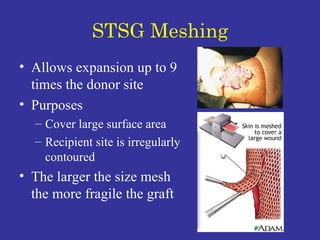
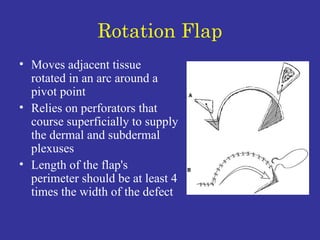
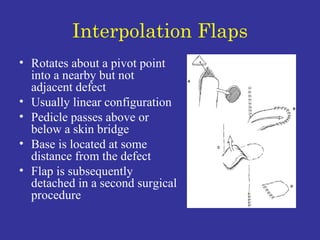
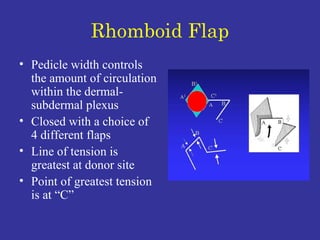
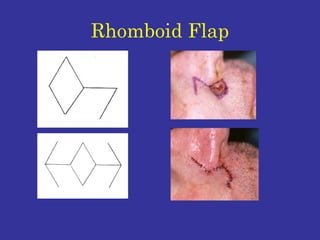
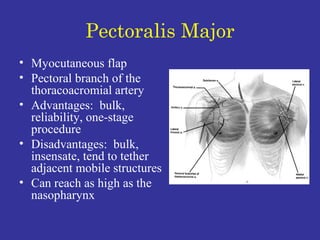
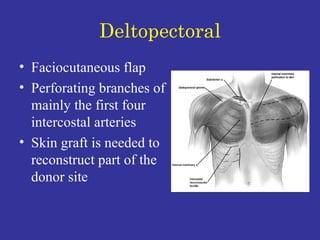
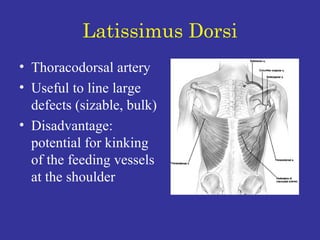
The document discusses various types of skin grafts and flaps used in head and neck reconstruction. It describes skin grafts such as split-thickness skin grafts (STSG) and full-thickness skin grafts (FTSG), and how they are harvested. It also discusses different types of flaps based on their blood supply patterns (random or axial), methods of transfer (advancement, transposition, rotation), configurations (rhomboid, bilobed), and locations (local, regional, distant). Common regional flaps used in head and neck reconstruction like pectoralis major, deltopectoral, and latissimus dorsi flaps are also described.






















































































![784cdysphonia[1]](https://cdn.slidesharecdn.com/ss_thumbnails/784cdysphonia1-1234158878157310-2-thumbnail.jpg?width=640&height=640&fit=bounds)




















![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)





