Downloaded 118 times



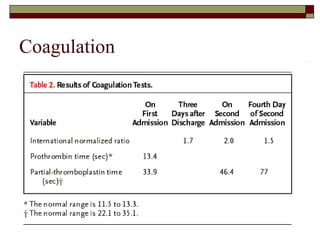
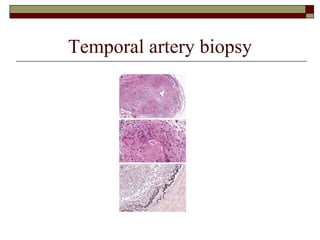
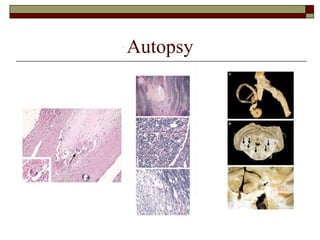
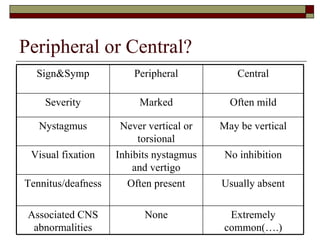


This document summarizes a case study of a 72-year-old man admitted to the hospital with recurrent neurological symptoms including numbness, slurred speech, diplopia, and vertigo. Examination revealed slight gait imbalance. Imaging and tests did not reveal a cause. He was discharged on anticoagulants but readmitted a few days later with worsening symptoms. A temporal artery biopsy led to a diagnosis of giant cell arteritis. His condition continued to deteriorate and he passed away. The document then provides an overview of balance disorders, types of vertigo, approaches to diagnosis of dizziness, and treatments.





















































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


















