Downloaded 234 times


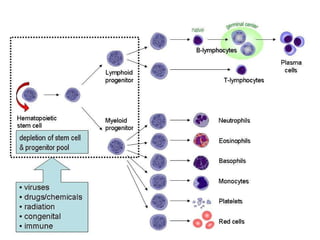
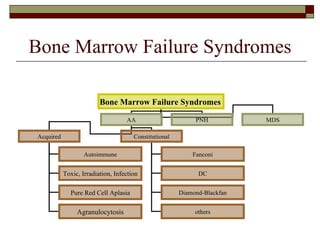
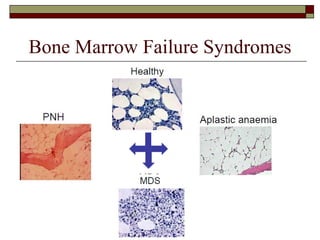
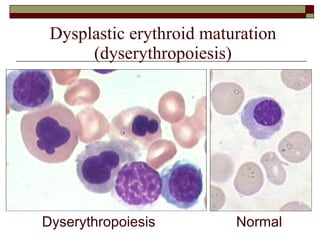
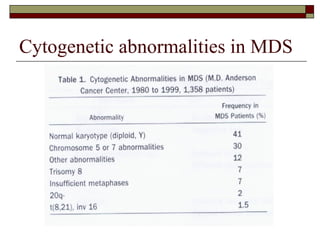
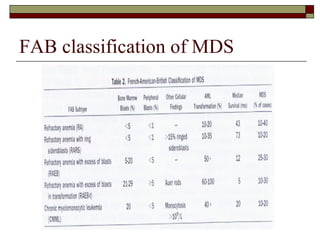



Myelodysplasia, also known as myelodysplastic syndrome (MDS), is a heterogeneous group of hematopoietic stem cell disorders that results in ineffective hematopoiesis and cytopenias. MDS is primarily seen in elderly patients and has a risk of progression to acute myeloid leukemia. Characteristic features include increased marrow proliferation, failure of stem cells to differentiate, and increased marrow apoptosis. Cytogenetic abnormalities are detected in 30-70% of patients and correlate with risk of progression. Treatment may include stem cell transplant, DNA methyltransferase inhibitors, immunotherapy, and chemotherapy.



















































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)








![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)