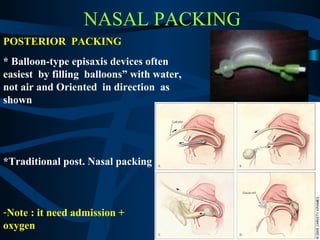
This document provides an overview of epistaxis (nosebleeds), including causes, locations, clinical approach, and management. It notes that epistaxis affects 5-10% of the population annually and can originate from the nose, nasopharynx, paranasal sinuses, or anterior cranial fossa. Local causes include trauma, inflammation, and tumors, while systemic causes involve conditions like hypertension, coagulopathies, and liver/kidney disease. Anterior nosebleeds are more common and originate from Little's area, while posterior bleeds originate from the sphenopalatine artery. Clinical assessment involves history, exam, and identifying the bleeding site. Management includes vasoconstrictors, caut