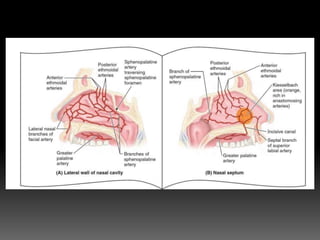
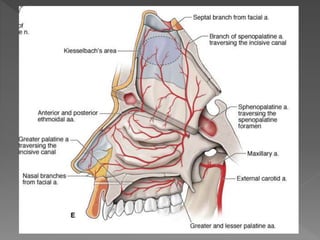
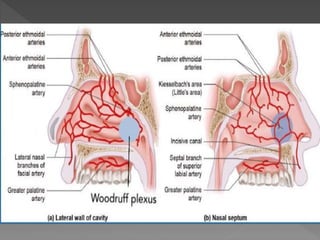
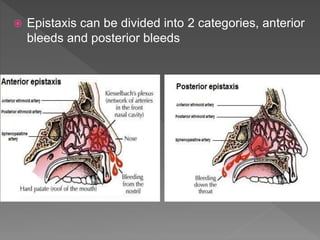
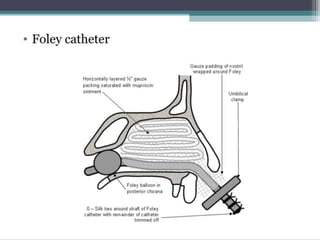
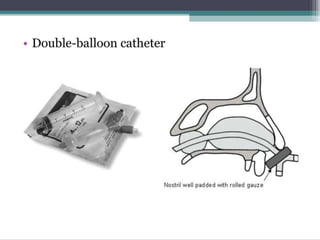
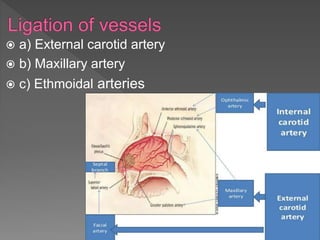
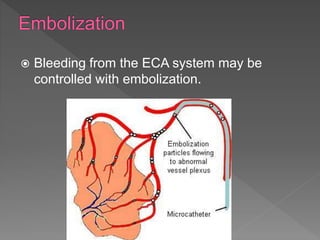
This document discusses epistaxis (nosebleeds), including its definition, causes, pathophysiology, and management. It notes that nosebleeds can be anterior or posterior based on the source of bleeding within the nasal cavities and outlines the various blood vessels involved. Common causes include trauma, inflammation/infection, tumors, hypertension, and medications. Management involves first aid, cauterization, nasal packing, and potentially surgical intervention. Prevention focuses on controlling risk factors and avoiding behaviors that could cause trauma to nasal tissues.