Downloaded 3,481 times


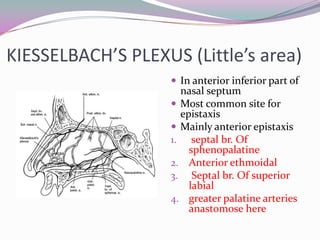





















This document discusses epistaxis (nosebleeds), including: 1. Epistaxis is bleeding from the nasal cavity and can occur in all age groups, though it is most common in children and young adults. The nasal cavity has a rich blood supply making it prone to bleeding. 2. Common causes of anterior epistaxis include local trauma, inflammation, infections, and physiological factors like climate. Systemic causes include hypertension, liver/kidney disease, and coagulation disorders. 3. Treatment begins with first aid and locating the bleeding site. Definitive treatments include chemical or electrocautery, vasoconstrictor sprays, and anterior nasal packing. Refractory epist



































































