Downloaded 641 times

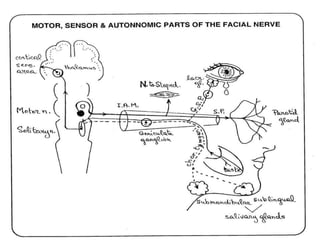

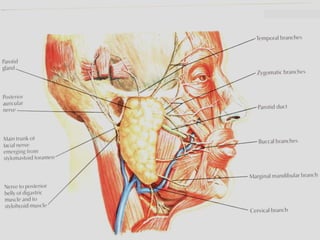
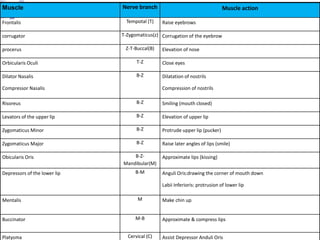
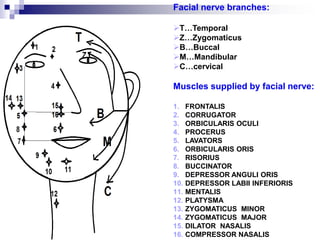
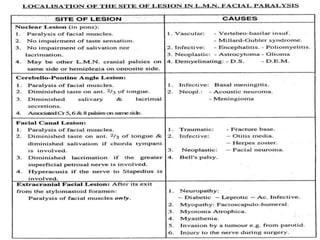
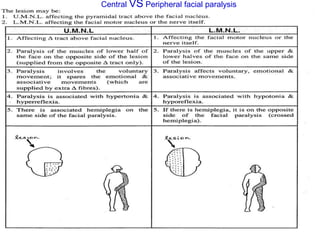
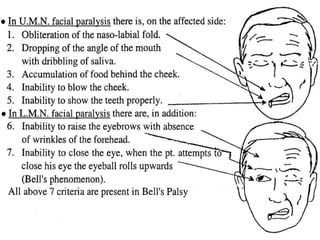
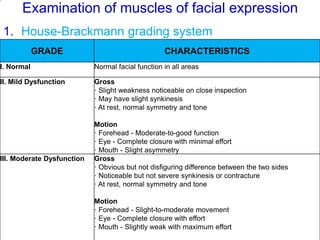
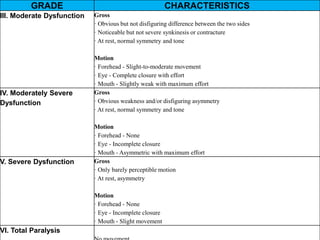
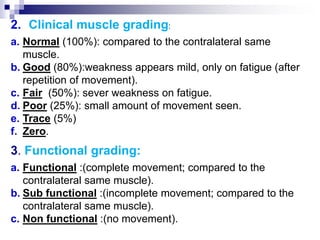
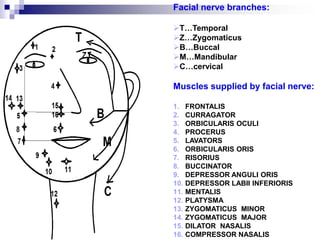





This document discusses facial nerve paralysis, including: - The anatomy of the facial nerve and branches that innervate facial muscles. - Common causes of facial nerve paralysis like Bell's palsy. - Evaluating facial nerve paralysis through examining facial muscles, taste sensation, lacrimation, and nerve conduction velocity. - Treating facial nerve paralysis with physical therapy including heat, electrotherapy, exercises and occasionally splinting.























































































