Downloaded 248 times









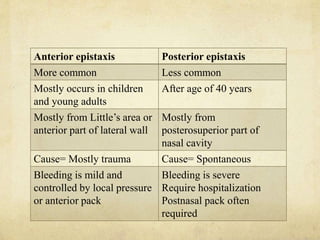





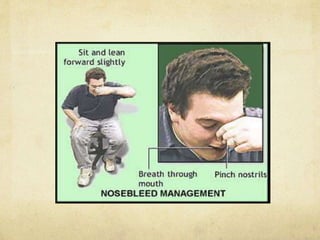



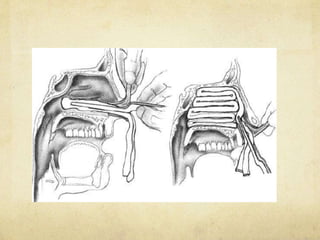




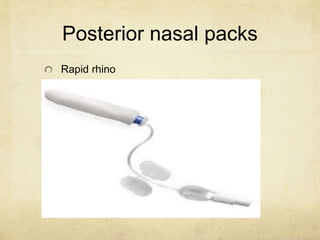
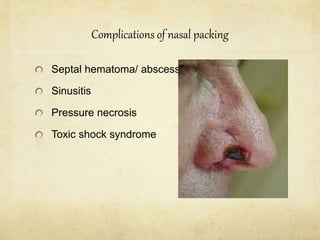

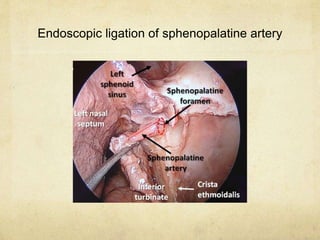







Epistaxis, or nosebleeds, can be caused by local factors within the nose or systemic factors elsewhere in the body. The vascular supply and common bleeding sites within the nose are described. Epistaxis is classified as anterior or posterior depending on the location of bleeding. Initial treatment involves local pressure and examination to locate the source before proceeding to cauterization, nasal packing, or other measures. Surgical ligation of arteries or angiographic embolization may be needed for severe or recurrent bleeding. Guidelines for managing epistaxis in children emphasize expectant treatment for mild cases over invasive procedures.



































































