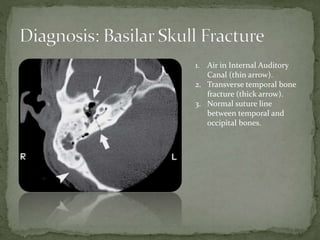
A 33-year-old woman presented to the emergency department after being struck behind the right ear by a flying baseball bat at a baseball game. She reported pain, tinnitus, dizziness, and slurred speech but denied loss of consciousness or nausea. Examination revealed right facial motor weakness, tenderness over the right mastoid bone, and right hemotympanum. CT scan showed a transverse temporal bone fracture and air in the internal auditory canal, consistent with a basilar skull fracture.