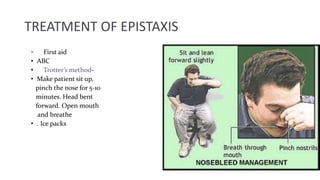
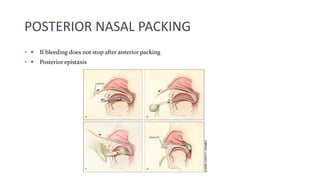
This document discusses the causes, management, and treatment of epistaxis (nosebleeds). Epistaxis is common and usually minor but can sometimes be severe or life-threatening. The nasal cavities have a rich blood supply which makes them susceptible to bleeding. Common causes include local trauma, inflammation, hypertension, and coagulation disorders. Treatment involves locating the bleeding site, cauterization, nasal packing, and controlling any underlying systemic issues. More severe cases may require arterial ligation or embolization procedures.