Download to read offline


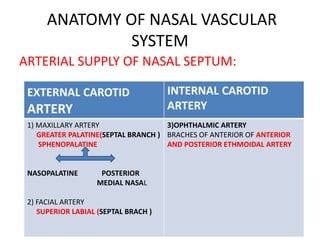
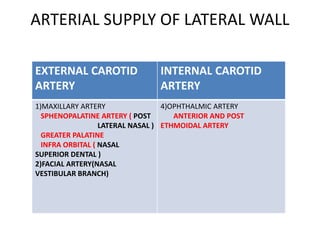
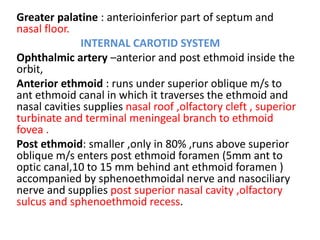
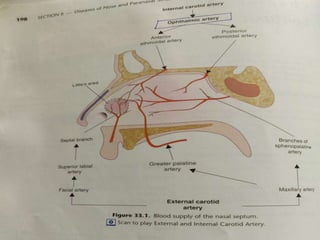
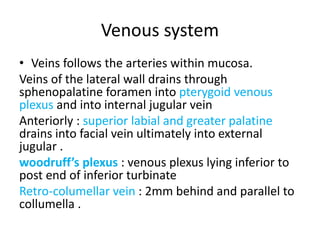
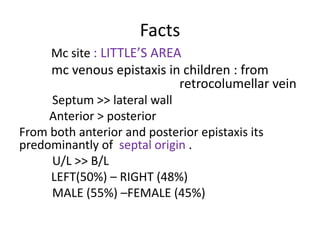
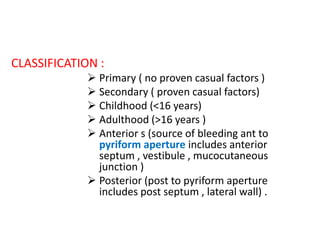
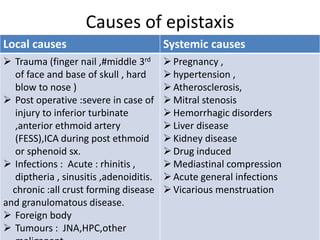
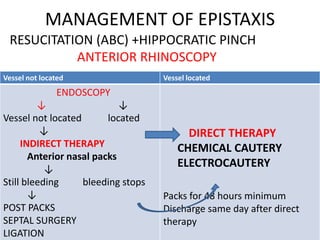
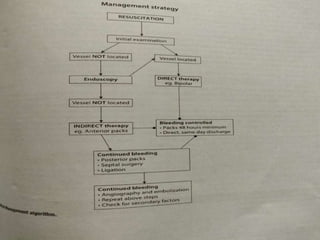
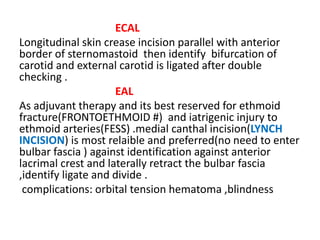
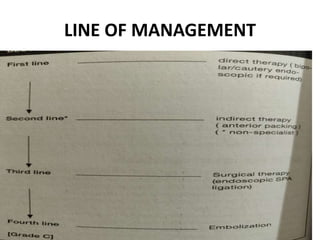

Epistaxis, or nosebleeds, are common. The nasal septum and lateral nasal wall receive their blood supply from branches of the external and internal carotid arteries. The most common site of bleeding is an area on the anterior nasal septum called Kiesselbach's plexus. Epistaxis can be classified as anterior or posterior based on the bleeding site. Causes include local trauma, infections, hypertension, and medications. Management involves direct therapies like cauterization to locate and treat the bleeding site or indirect therapies like nasal packing if the site cannot be identified. Refractory cases may require surgical ligation of arteries or embolization.


















































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
















