Downloaded 16 times
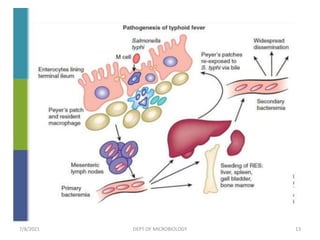
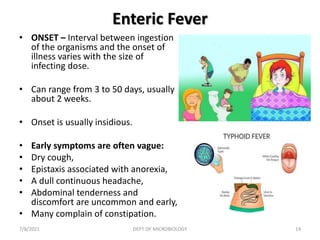
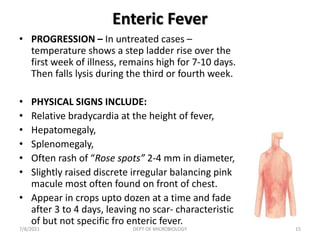
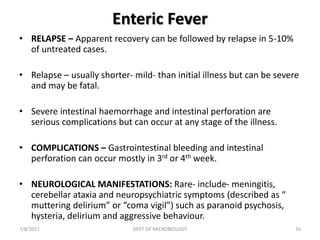


This document provides information on a lecture about enteric fever: 1. Enteric fever is caused by Salmonella typhi and Salmonella paratyphi, and causes a systemic illness characterized by fever, headache, and abdominal discomfort. It is transmitted through contaminated food and water. 2. Salmonella enters the intestines and adheres to the gut mucosa. It can then invade intestinal cells and enter the bloodstream, spreading to other organs and tissues. 3. Symptoms of enteric fever include a fluctuating fever that rises over the first week, hepatomegaly, splenomegaly, and rose colored spots on the chest. Without treatment, relapses can occur in 5























































































