Downloaded 640 times
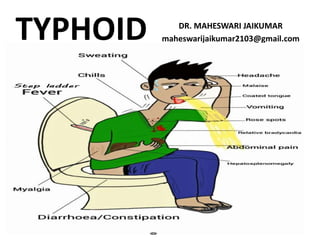
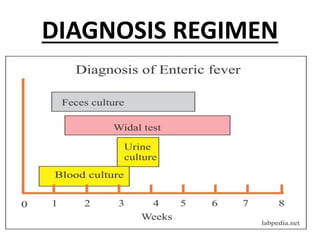





- Typhoid fever is caused by the bacterium Salmonella typhi and is transmitted through contaminated food or water. It causes a high fever that lasts 2-3 weeks along with gastrointestinal symptoms. - Chronic carriers who continue to shed the bacteria in their feces or urine can spread typhoid for many years and are difficult to treat. Proper sanitation, water treatment, handwashing, and vaccination programs are needed to control typhoid outbreaks. - Two vaccines are available - the Vi polysaccharide vaccine given as a single dose to individuals over 2, and the live attenuated Ty21a vaccine given orally in 3 doses over a week to individuals over 5. Vaccination provides protection for 3 years against