Downloaded 38 times
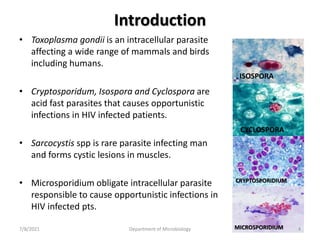
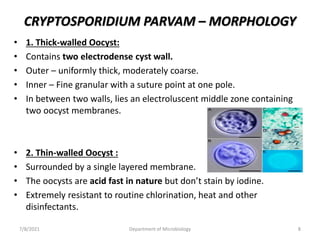
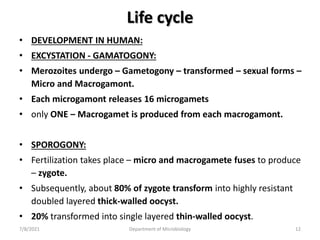
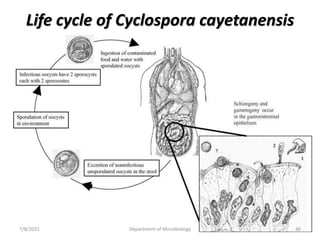
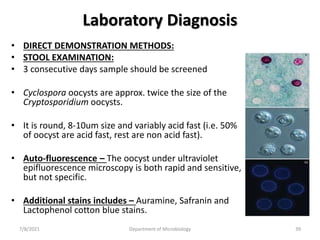

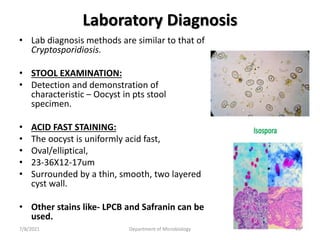


The document discusses coccidian parasites, with a focus on Cryptosporidium parvum. It describes the parasite's morphology, life cycle, epidemiology, pathogenesis, and clinical features. Cryptosporidium parvum causes cryptosporidiosis, an intestinal illness that typically results in self-limiting diarrhea but can cause serious, chronic diarrhea in immunocompromised patients like those with HIV/AIDS. Laboratory diagnosis involves examining stool samples microscopically to identify the parasite's oocysts.




















































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


