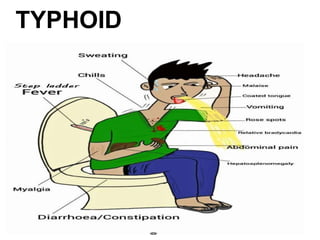
Typhoid fever is caused by the bacterium Salmonella typhi. It is transmitted through the fecal-oral route by ingesting food or water contaminated by the feces or urine of infected individuals. Clinical features include a sustained high fever over 2-3 weeks along with relative bradycardia and abdominal tenderness. Diagnosis is confirmed through blood or stool cultures. Treatment involves antibiotics such as fluoroquinolones. Control relies on identifying and treating carriers, improving sanitation and access to clean water, and administering vaccines to at-risk populations.