Downloaded 2,186 times
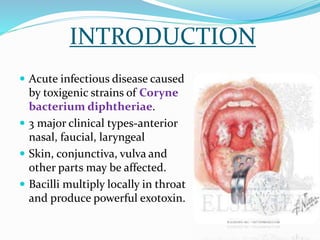






This document provides an overview of diphtheria including its introduction, history, epidemiology in India and worldwide, clinical features, diagnosis, treatment, immunization, and control. It notes that diphtheria is caused by Corynebacterium diphtheriae and presents as respiratory or cutaneous infection. While immunization has reduced cases in developed countries, it remains endemic in India and other developing areas due to lack of widespread vaccination. Treatment involves antitoxin and antibiotics. Control relies on maintaining high immunization coverage with DPT vaccine along with identifying and treating cases and carriers.











































































