The document discusses poliomyelitis (polio), including:
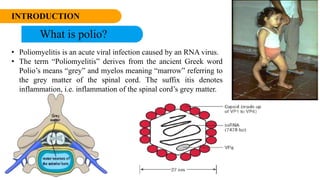
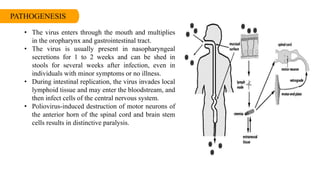
- Polio is an acute viral infection caused by poliovirus that can cause paralysis. It is transmitted through the fecal-oral route or droplets.
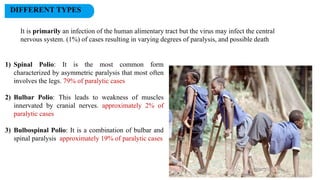
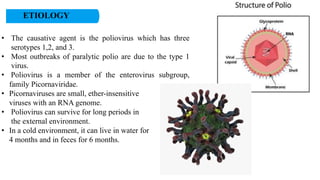
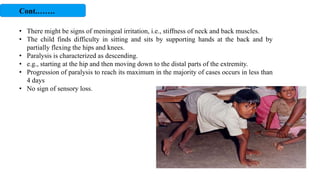
- There are three types of poliovirus. Infection results in subclinical, abortive, non-paralytic, or paralytic cases. Paralysis occurs when the virus infects motor neurons in the spinal cord.
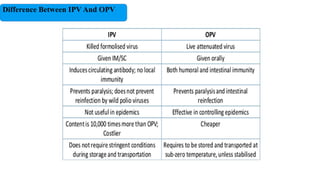
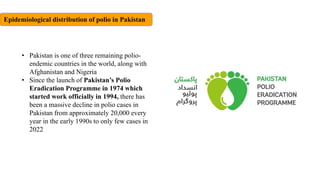
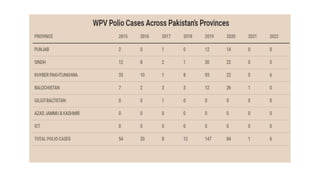
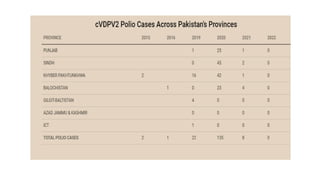
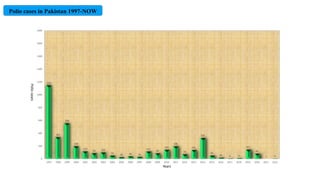
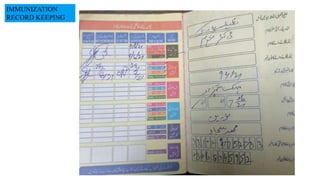
- Pakistan saw over 1,000 polio cases in 1997 but improved vaccination programs have reduced this to single digits by 2022. Oral and inactivated polio vaccines are used to prevent transmission and eradicate the disease.








































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)













