Downloaded 157 times
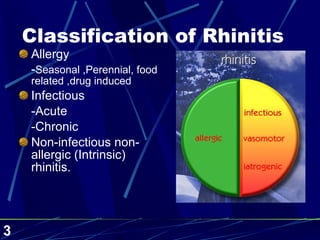
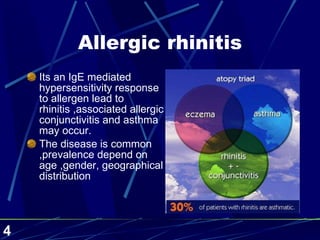


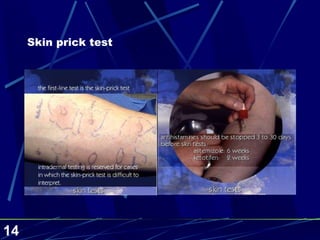
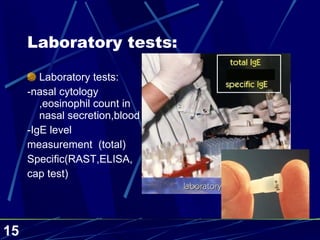
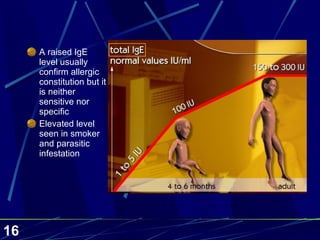
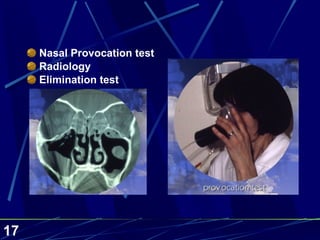
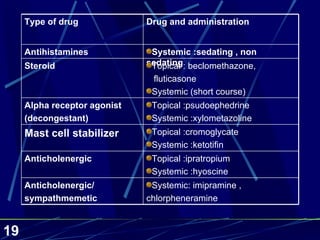
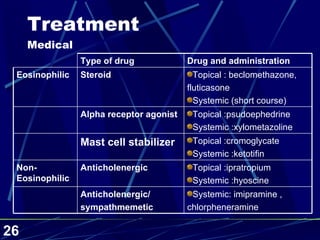
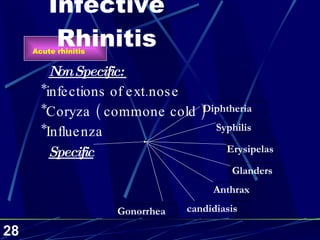
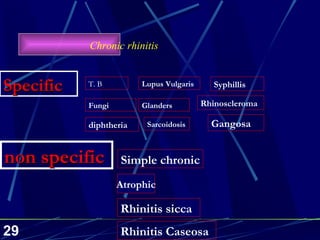



Rhinitis is inflammation of the nasal cavity lining. It can be classified as allergic, infectious, or non-infectious non-allergic. Allergic rhinitis is an IgE-mediated response to allergens like pollen, dust mites, or animal dander. Symptoms include sneezing, runny nose, and nasal obstruction. Treatment involves avoidance of allergens, medications like antihistamines, nasal steroids, and immunotherapy. Infectious rhinitis can be acute or chronic and caused by bacteria, viruses, or fungi. Non-allergic rhinitis may be due to intrinsic factors, drugs, hormonal changes, or rebound from nasal decon













































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)









