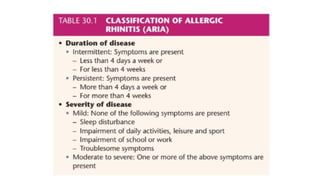
Allergic rhinitis, also known as hay fever, is an inflammatory disorder of the nasal passages caused by airborne allergens, with symptoms varying by type (seasonal or perennial). Treatment includes allergen avoidance, medications (like antihistamines and corticosteroids), and immunotherapy, while investigations may involve tests for eosinophilia and specific IgE measurements. Vasomotor rhinitis is a nonallergic condition mimicking allergic rhinitis, characterized by nasal congestion and rhinorrhea, managed through avoidance of triggers and medications.