Downloaded 450 times
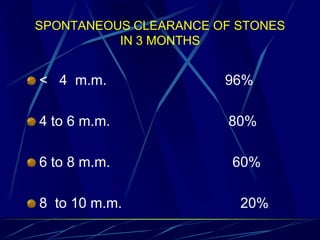
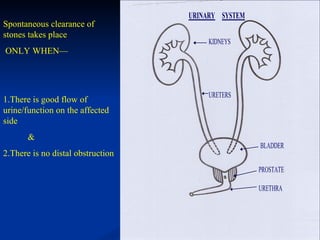
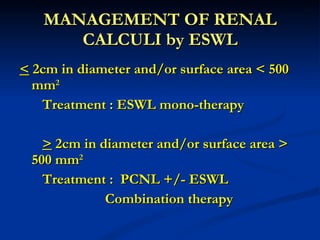



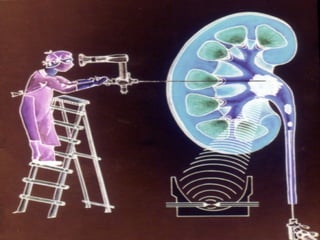

























The document discusses different treatment options for renal and ureteric stones, including conservative management, extracorporeal shock wave lithotripsy (ESWL), percutaneous nephrolithotomy (PCNL), ureteroscopy (URS), and open surgery. For renal stones less than 2cm, ESWL is recommended, while PCNL may be used for larger stones or when ESWL fails. URS is recommended for ureteric stones, with an 85-90% success rate in achieving a stone-free state. Complications, prevention strategies, and dietary and medication advice are also summarized.




































![Urinary Stone Management [Dr. Edmond Wong]](https://cdn.slidesharecdn.com/ss_thumbnails/stonemanagementedmond-140716213042-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)















![Urolithiasis presented by Dr Muhammad nouman([Autosaved]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/urolithiasisautosaved-1-250603143258-c924c676-thumbnail.jpg?width=640&height=640&fit=bounds)






















































