Downloaded 2,030 times



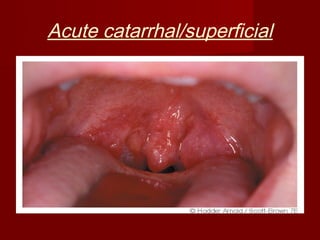






This document discusses the anatomy, causes, symptoms, diagnosis and treatment of tonsillitis. It describes the anatomy of the palatine tonsils and their location in the oropharynx. It explains that tonsillitis is commonly caused by bacterial or viral infections, and presents as sore throat, difficulty swallowing and fever. The types of acute tonsillitis - catarrhal, follicular and membranous - are outlined. Treatment involves rest, fluids, analgesics and antibiotics. Complications and differential diagnoses are also summarized.





































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)

















