Downloaded 128 times
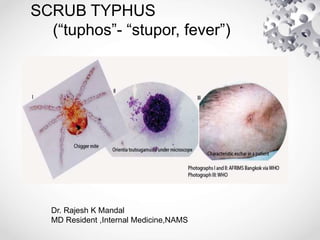





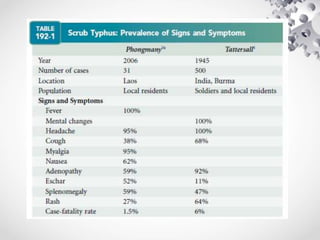

Scrub typhus is caused by the bacteria Orientia tsutsugamushi, which is transmitted through the bites of infected trombiculid mites. It causes an acute febrile illness with symptoms such as fever, headache, and rash. If left untreated, it can lead to complications affecting multiple organs and the case fatality rate is 7%. Diagnosis is made through serologic tests detecting antibodies or PCR detecting bacterial DNA. Treatment involves doxycycline or azithromycin antibiotics, with fever typically resolving within 1-2 days. Prevention involves wearing protective clothing, using insect repellent, and clearing vegetation to limit mite habitats.
















































































