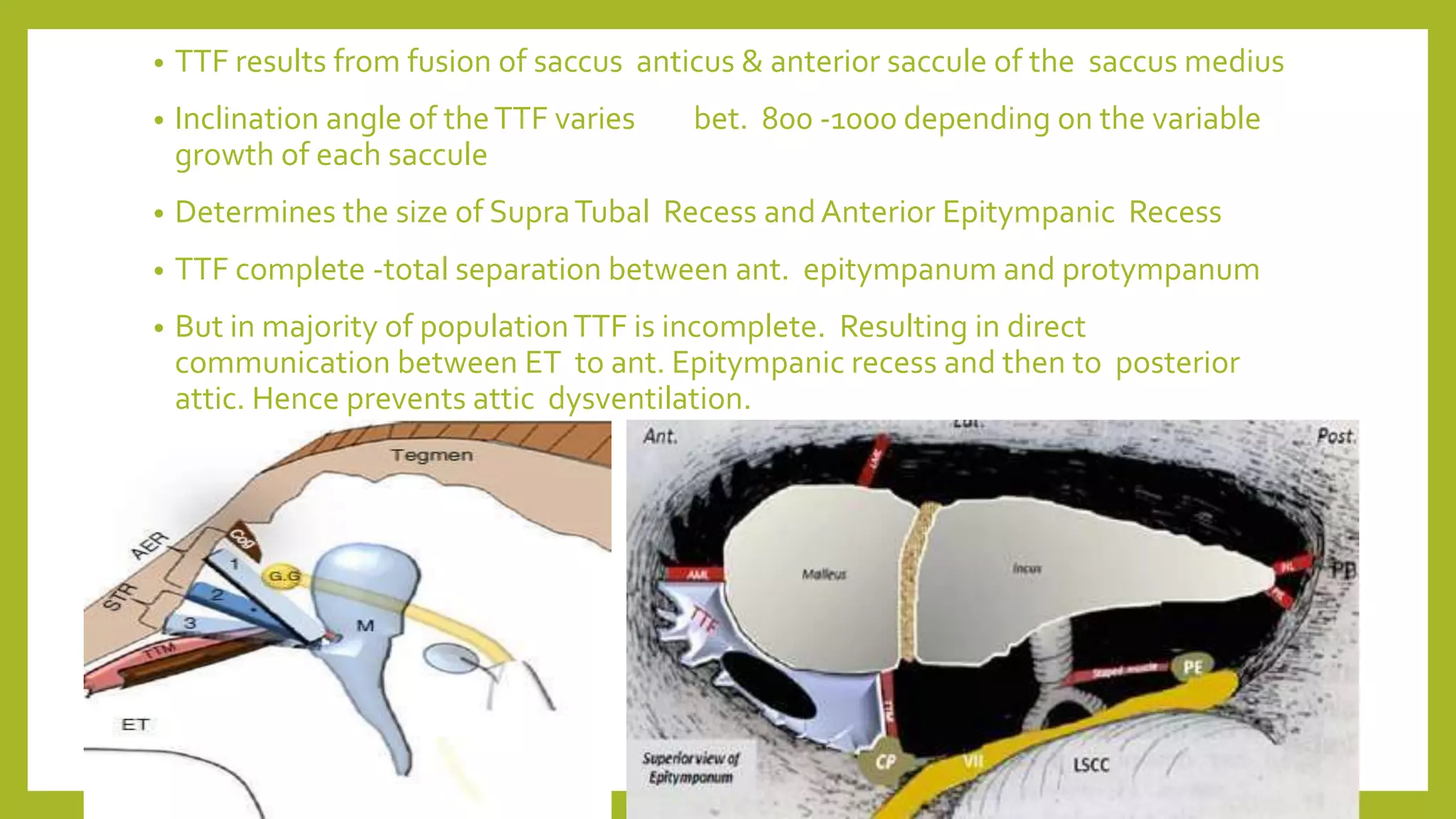
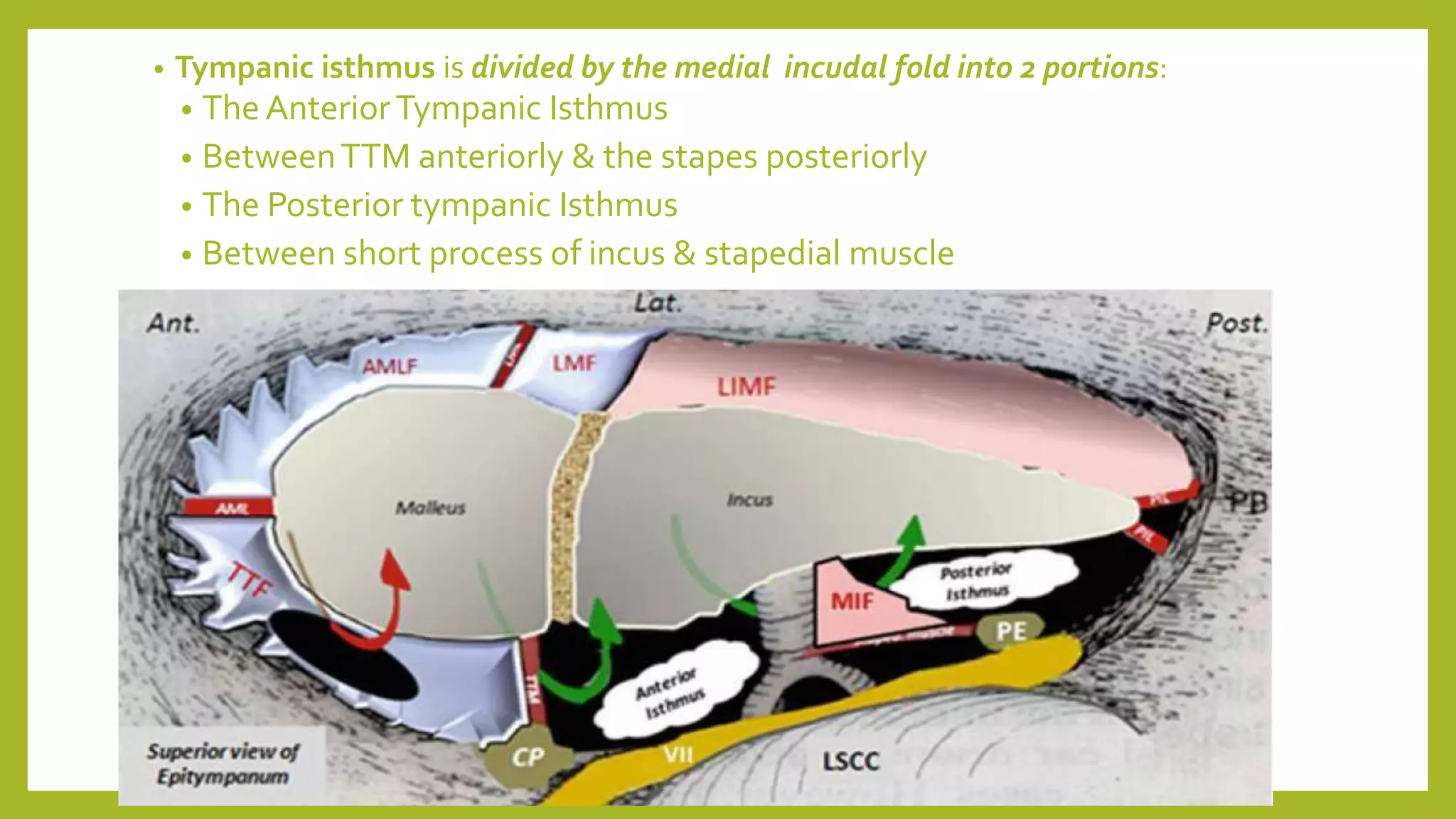
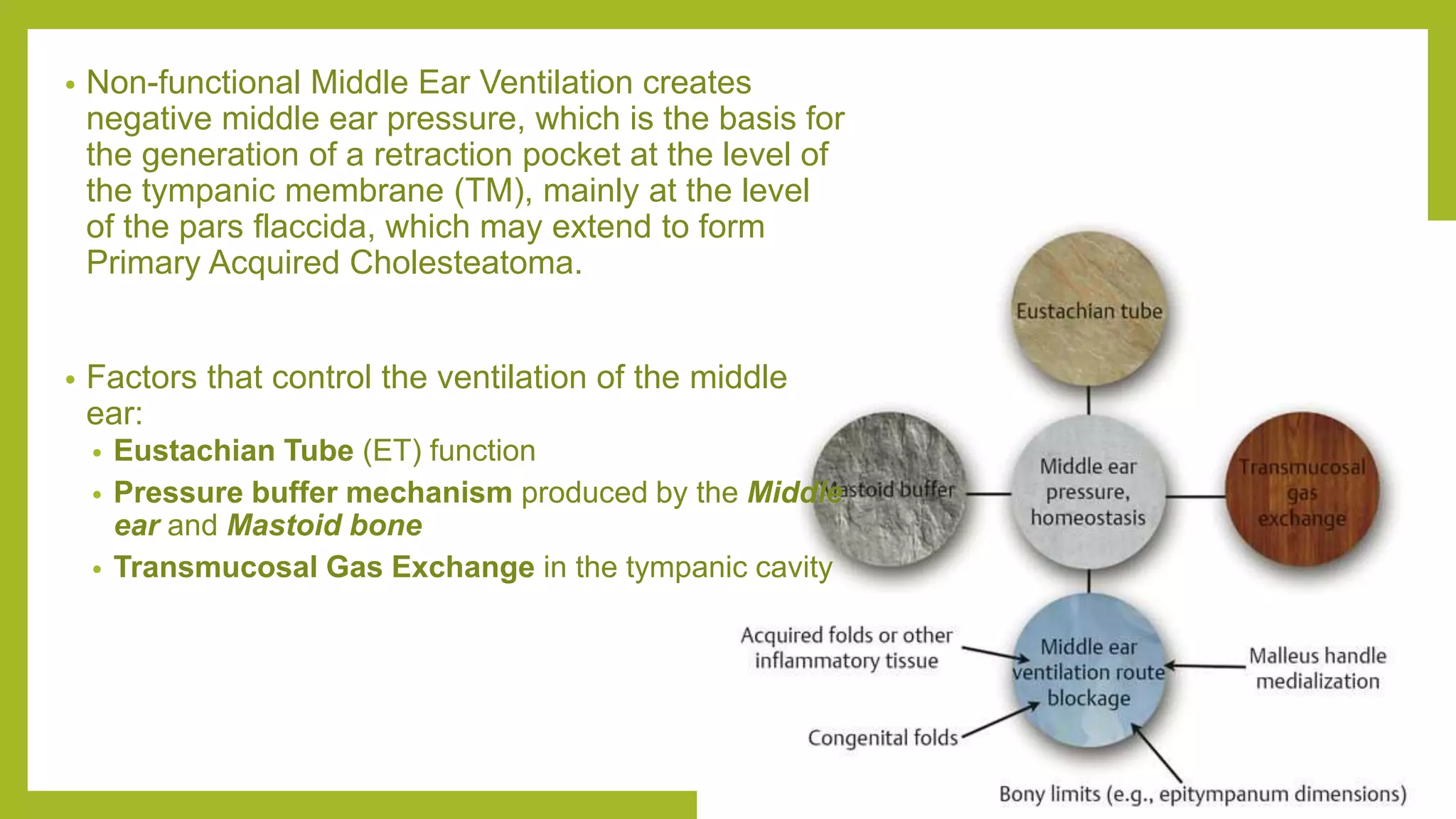
The document discusses the anatomy and physiology of the middle ear ventilation pathways. It describes the mucosal folds in the middle ear which develop during fetal development from sacs and pouches. Important folds include the tensor tympani fold, malleal folds, and incudal folds. These folds orient the spread of middle ear pathology. The tympanic isthmus and its blockage are also discussed, which can lead to attic dysventilation even with a normally functioning Eustachian tube. Preserving the tensor tympani fold during surgery is important to ensure ventilation of the attic region. A well-aerated mastoid and functioning Eustachian tube also help in maintaining proper middle ear ventilation


![Anatomy of the eustachian tube [Right ear]:
(a) The cartilaginous portion and related muscles
of the eustachian tube; posterior view
(b) The eustachian tube orifice: a view tangential
to the eustachian tube lumen at the level of the
rhinopharynx
(c) Bony and cartilaginous portions of the
eustachian tube, coronal view
tvpm- tensor veli palatini muscle
lvpm- levator veli palatine muscle
tuc- cartilaginous component of the eustachian
tube
psf- petrosphenoidal fissure
spcm- superior pharyngeal constrictor muscle
stl- suspensory tubal ligament](https://image.slidesharecdn.com/middleearventilatorypathwayandmucosalfolds-230301152220-825af022/75/Middle-ear-ventilatory-pathway-and-Mucosal-folds-pptx-5-2048.jpg)
![Total retraction of the eardrum in a patient with failure
of eustachian tube function: [Right ear]
(a) axial view at the epitympanic level
(b) coronal view
(c) sagittal view
In this case we observe a decrease of the pressure
throughout the middle ear and mastoid, with
subsequent retraction of the pars flaccida and pars
tensa.
in- incus; ma- malleus
s- stapes is- isthmus
tf- tensor fold fn- facial nerve
d- eardrum prs- Prussak space
imlf- lateral incudomalleal fold mlf- lateral malleal
fold
lsc- lateral semicircular canal cho- cochlea](https://image.slidesharecdn.com/middleearventilatorypathwayandmucosalfolds-230301152220-825af022/75/Middle-ear-ventilatory-pathway-and-Mucosal-folds-pptx-6-2048.jpg)



![Epitympanic diaphragm in a patient with a Complete tensor
fold: [Right ear]
Epitympanic diaphragm in a patient with an Incomplete
tensor fold: [Right ear]
s-stapes; fn-facial nerve; cp- cochleariform process; ma-
malleus;
in-incus; aes-anterior epitympanic compartment;
amf-anterior malleolar fold; pes-posterior epitympanic
compartment; pil-posterior incudal ligaments; tf-tensor fold; mlf-
lateral malleal fold; imlf-lateral incudomalleal fold; is-isthmus;
pe-pyramidal eminence.](https://image.slidesharecdn.com/middleearventilatorypathwayandmucosalfolds-230301152220-825af022/75/Middle-ear-ventilatory-pathway-and-Mucosal-folds-pptx-11-2048.jpg)
![Middle ear aeration pathway in a patient with
normal function of the eustachian tube: [Right
ear]
(a) axial view at the epitympanic level
(b) coronal view
(c) sagittal view
in, incus; ma, malleus; s, stapes; is, isthmus; tf,
tensor fold; fn, facial nerve; dr, eardrum; prs,
Prussak space; imlf, lateral incudomalleal fold;
mlf, lateral malleal fold; cho, cochlea; lsc, lateral
semicircular canal.](https://image.slidesharecdn.com/middleearventilatorypathwayandmucosalfolds-230301152220-825af022/75/Middle-ear-ventilatory-pathway-and-Mucosal-folds-pptx-12-2048.jpg)


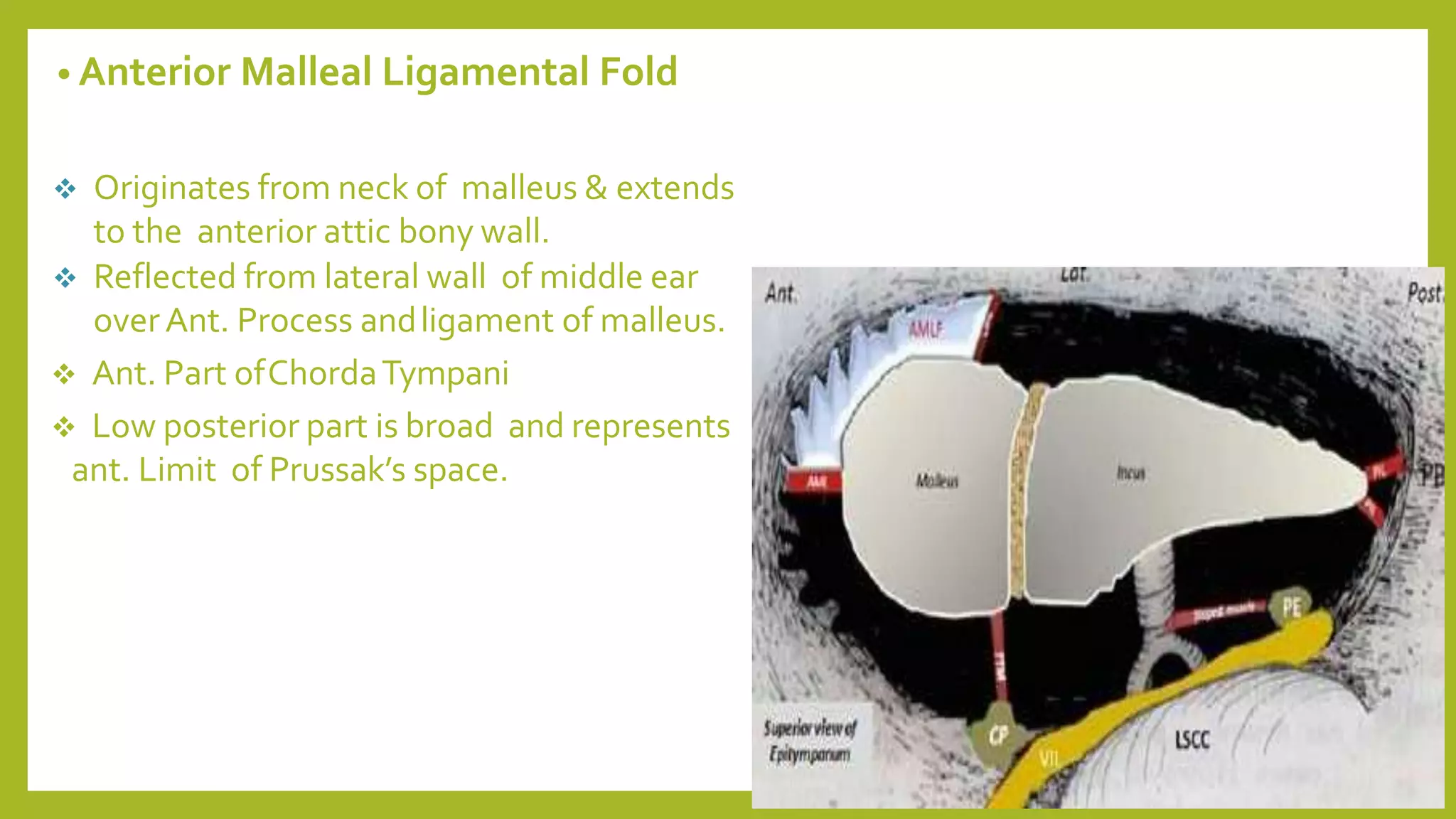
![ Mucosal folds extend from the wall of middle ear to its content & carry ligaments
and blood vessels to the ossicles.
These folds orient the progress of middle ear pathologies but are not true
barrier against their extension.
Mucosal folds [2 types]
Composite fold: Ligament+ Lining mucosa
[Ant.MLF, Lat.MLF, Post. Incudal fold]
Duplicate fold: fusion of two expanding air sac walls in absence of any
interposing structure.
[Tensor tympani fold, Lateral incudomalleal fold]](https://image.slidesharecdn.com/middleearventilatorypathwayandmucosalfolds-230301152220-825af022/75/Middle-ear-ventilatory-pathway-and-Mucosal-folds-pptx-16-2048.jpg)