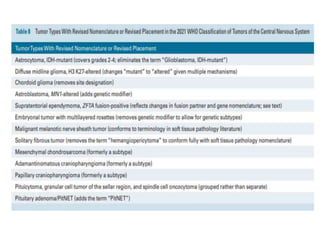
The 2021 WHO classification of CNS tumors builds on the 2016 edition by placing greater emphasis on molecular markers for both classification and grading. Some tumors are now entirely classified based on their molecular profile, while others remain primarily histologically assessed. A layered report structure will integrate histological, grading, and molecular information. Notable changes include raising IDH status and 1p19q codeletion to prominence for diffuse gliomas. Grading now occurs within each tumor type rather than equivalently across types. Molecular features can supersede histology in determining grade.
![Molecular grading
• For the first time, molecular features have been
explicitly added to the grading schema, and may
supersede histological features.
• For example, an IDH-wildtype astrocytoma with
low-grade histologic features can be considered
grade 4 (glioblastoma) in the presence of EGFR
amplification, TERT promoter mutation or the
combined gain of chromosome 7 and loss of
chromosome 10 [+7/-10]](https://image.slidesharecdn.com/cns2021classification-230205142548-0bea0043/85/CNS-WHO-2021-tumor-classification-pptx-9-320.jpg)