Downloaded 1,323 times










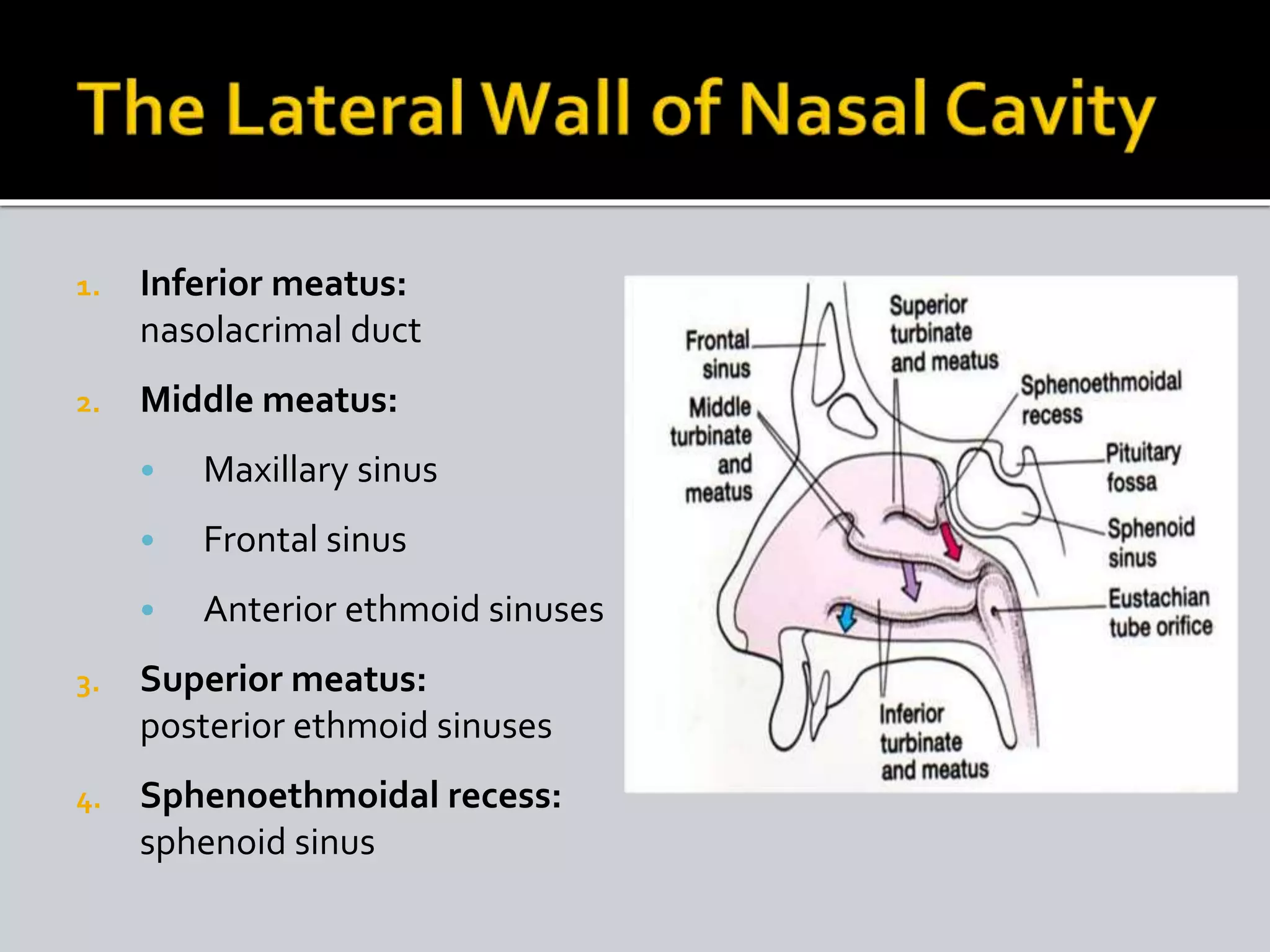


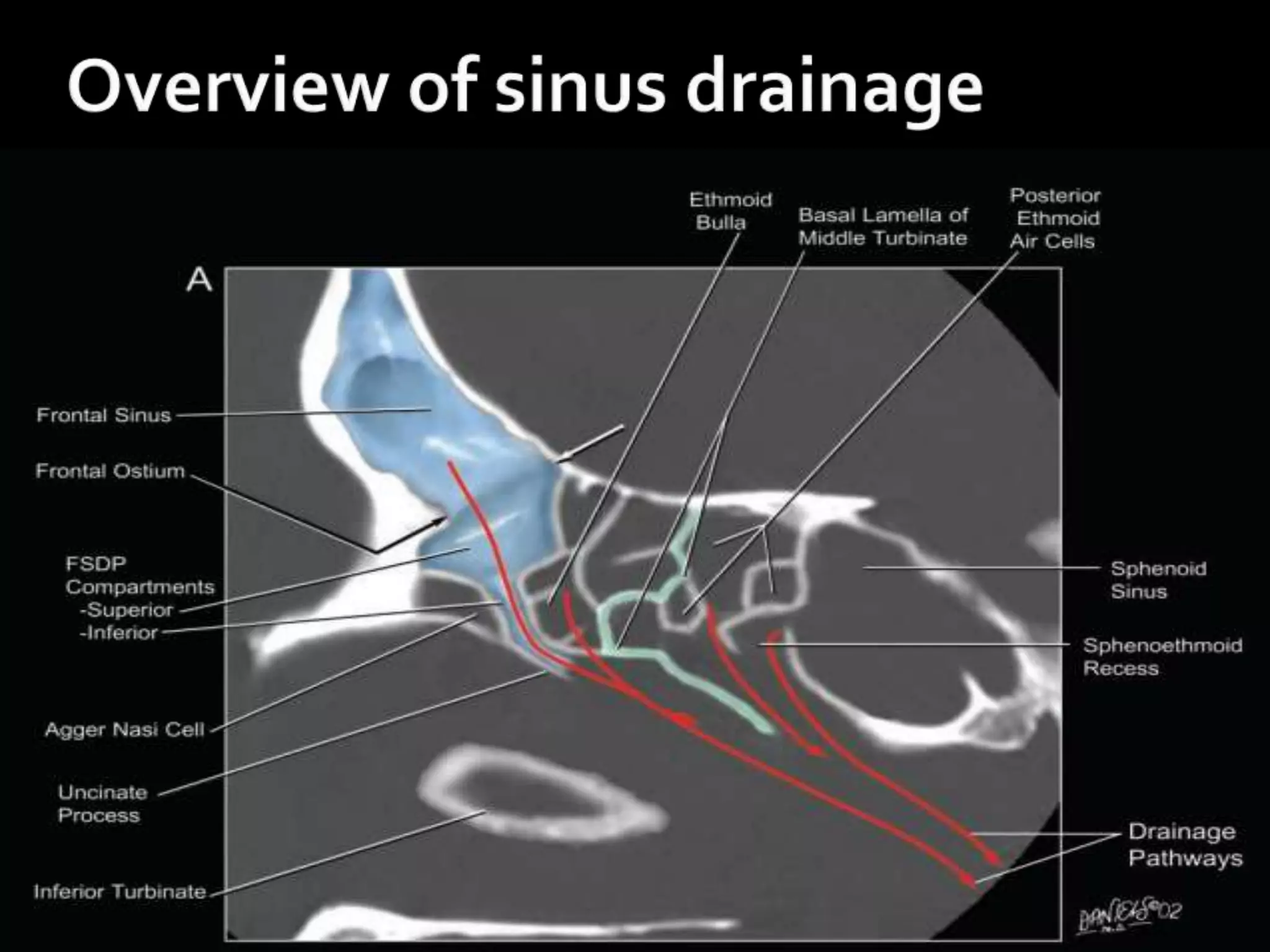


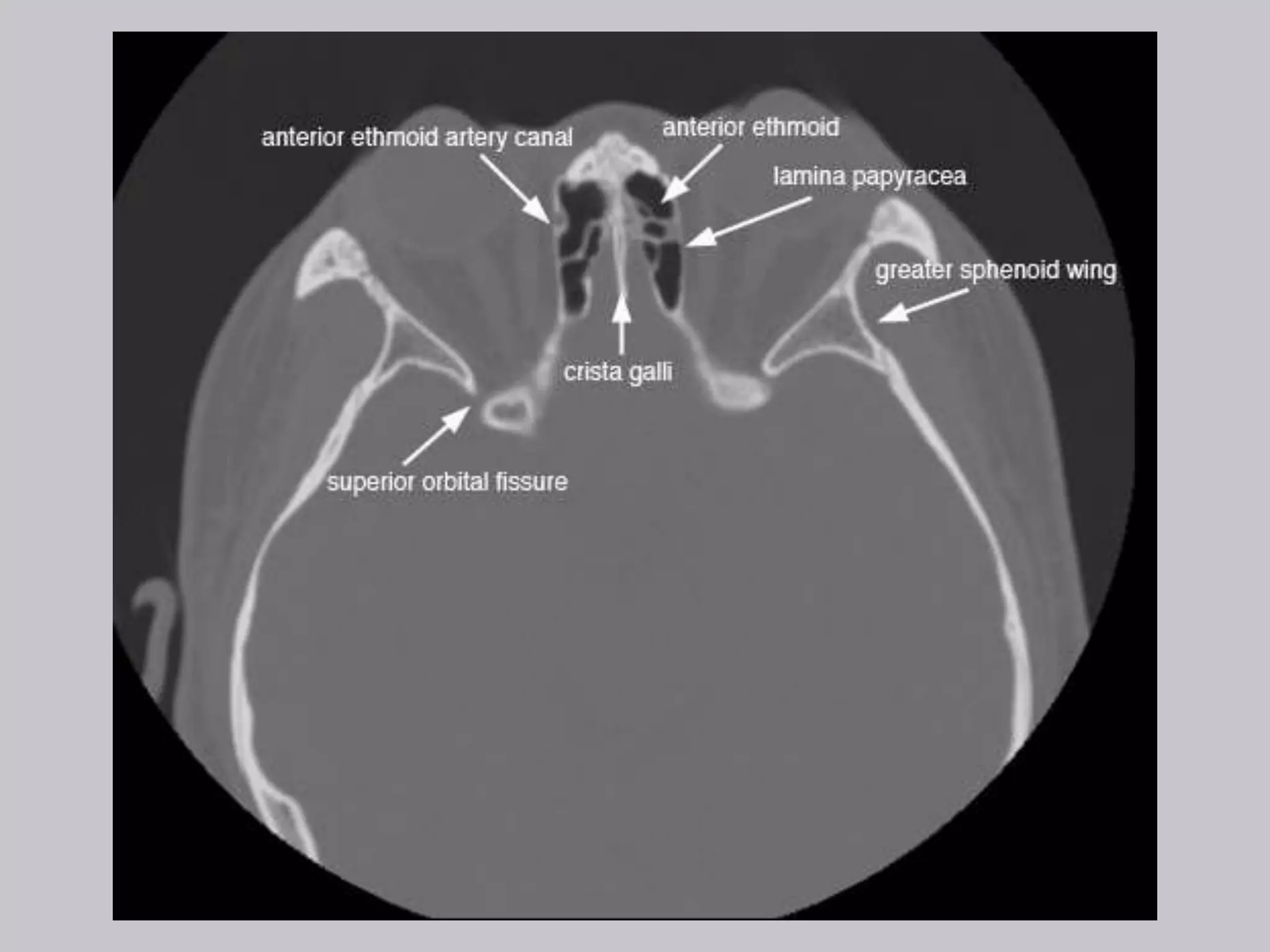






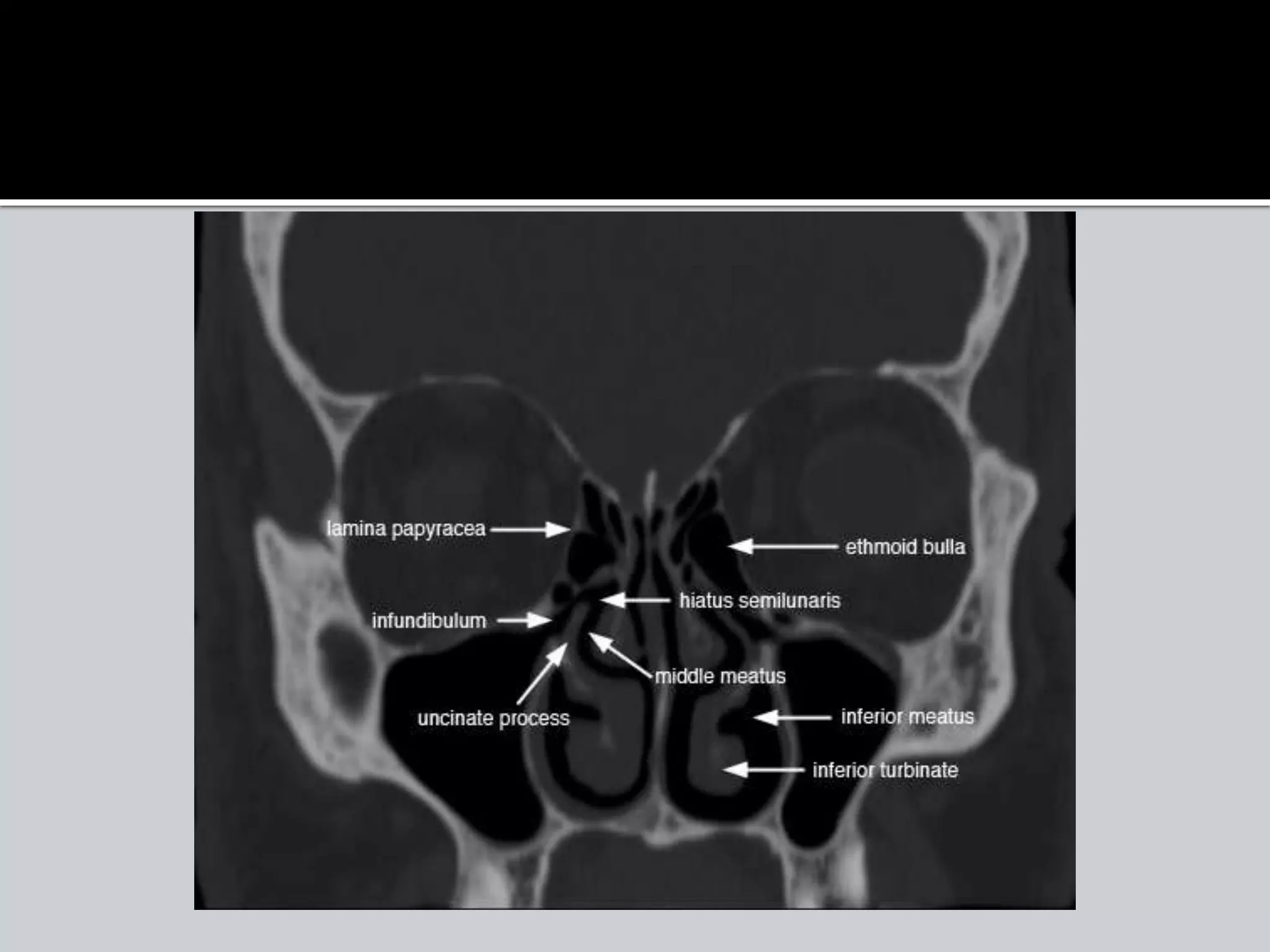






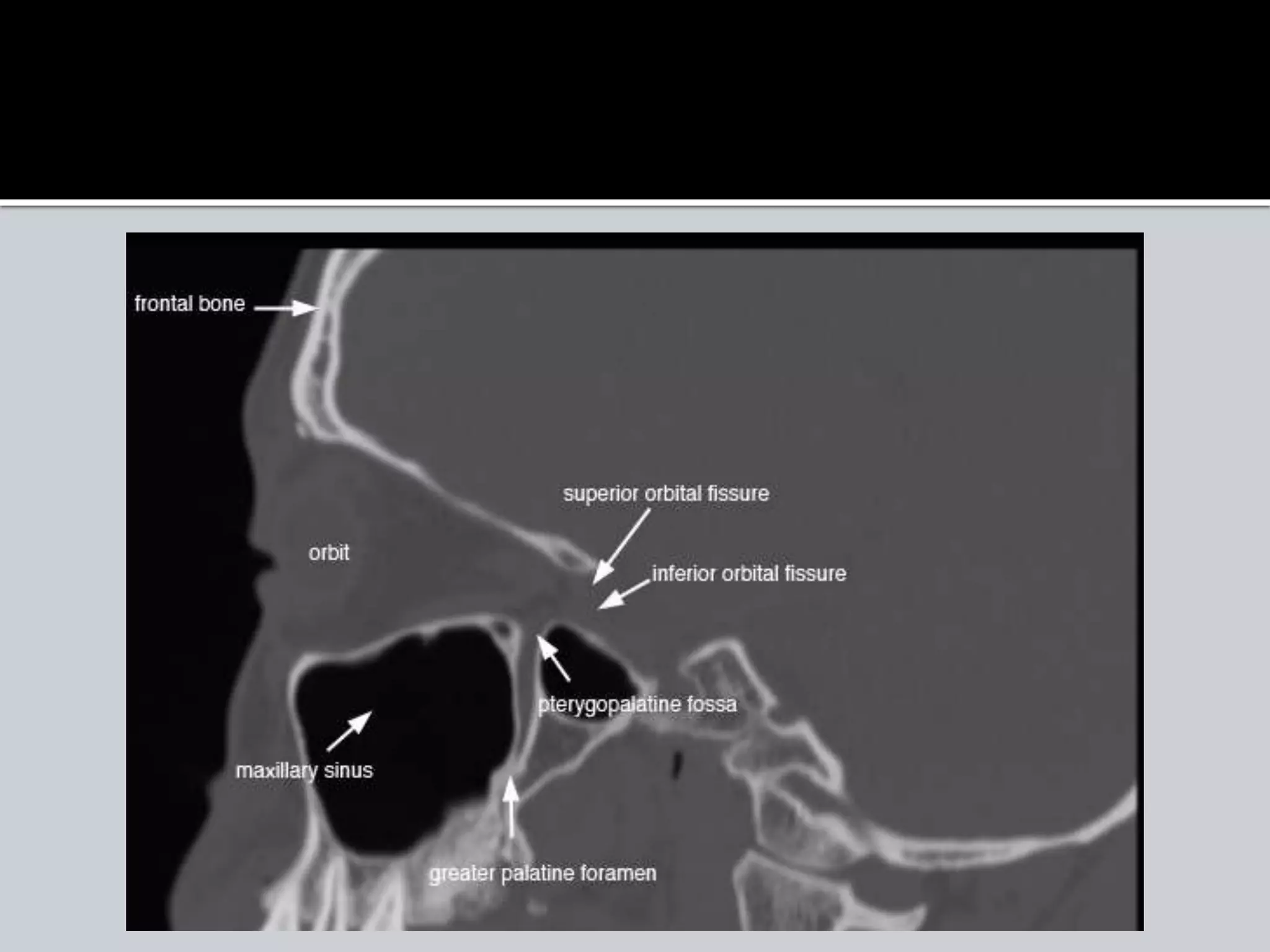
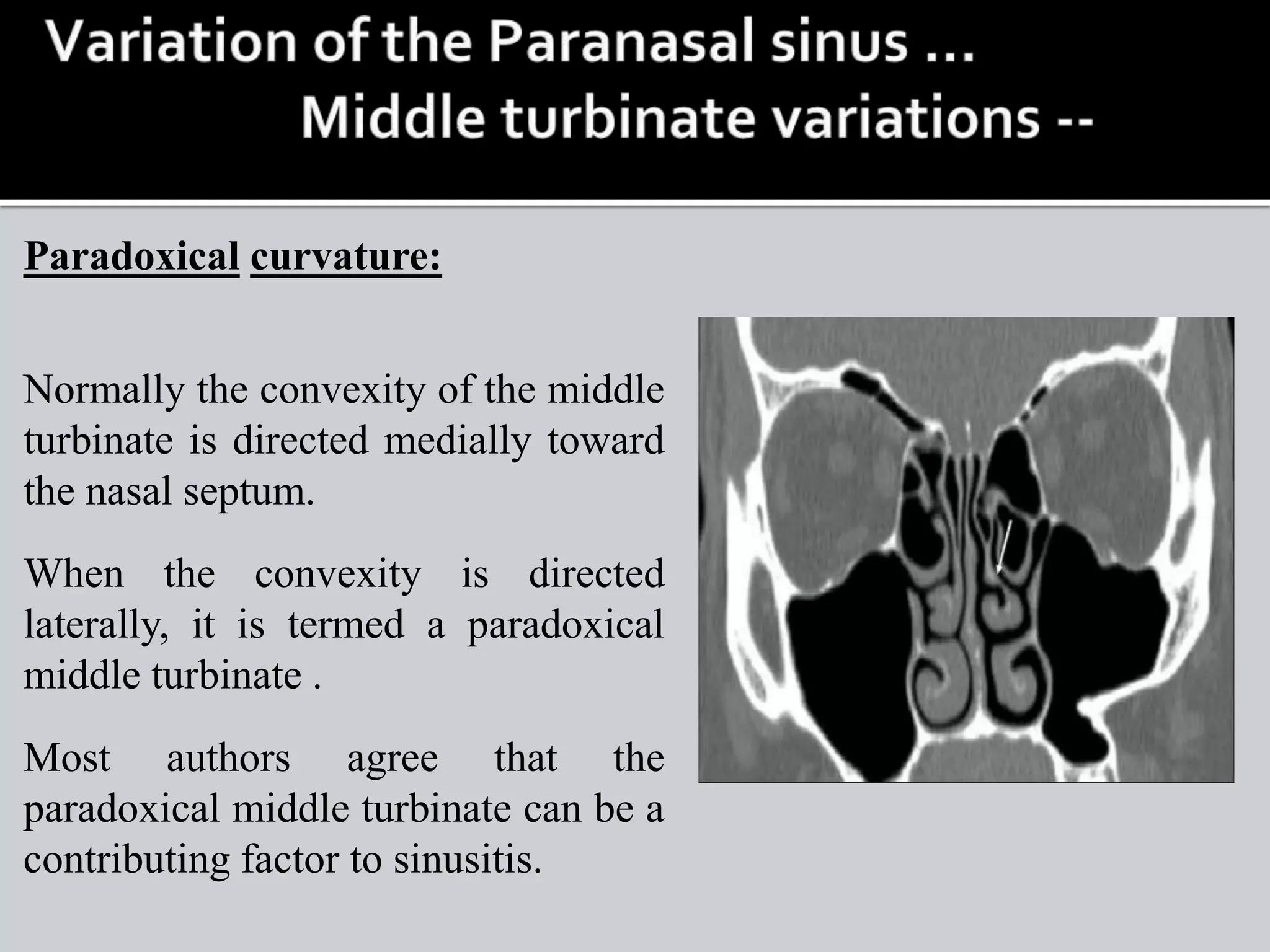
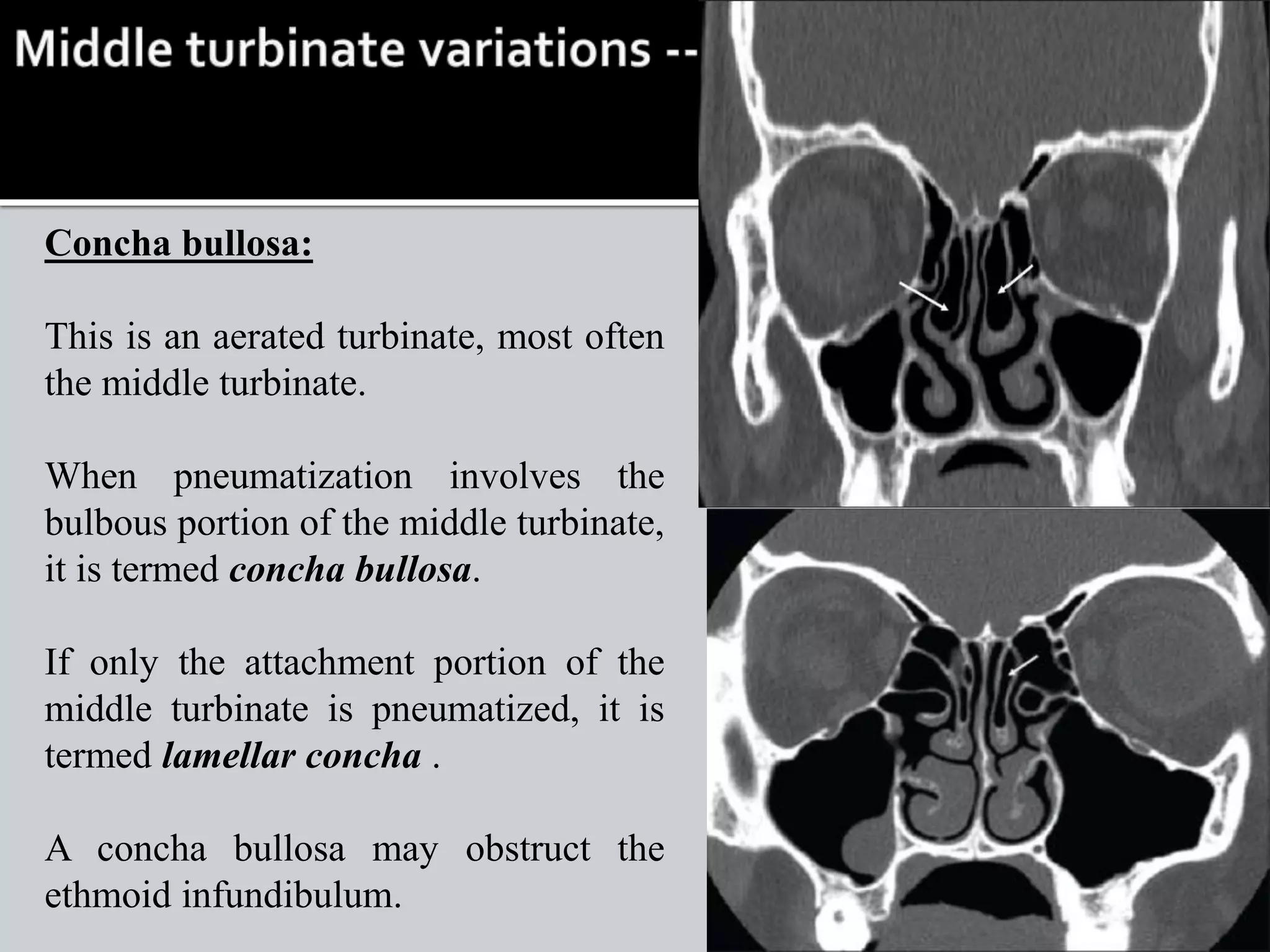
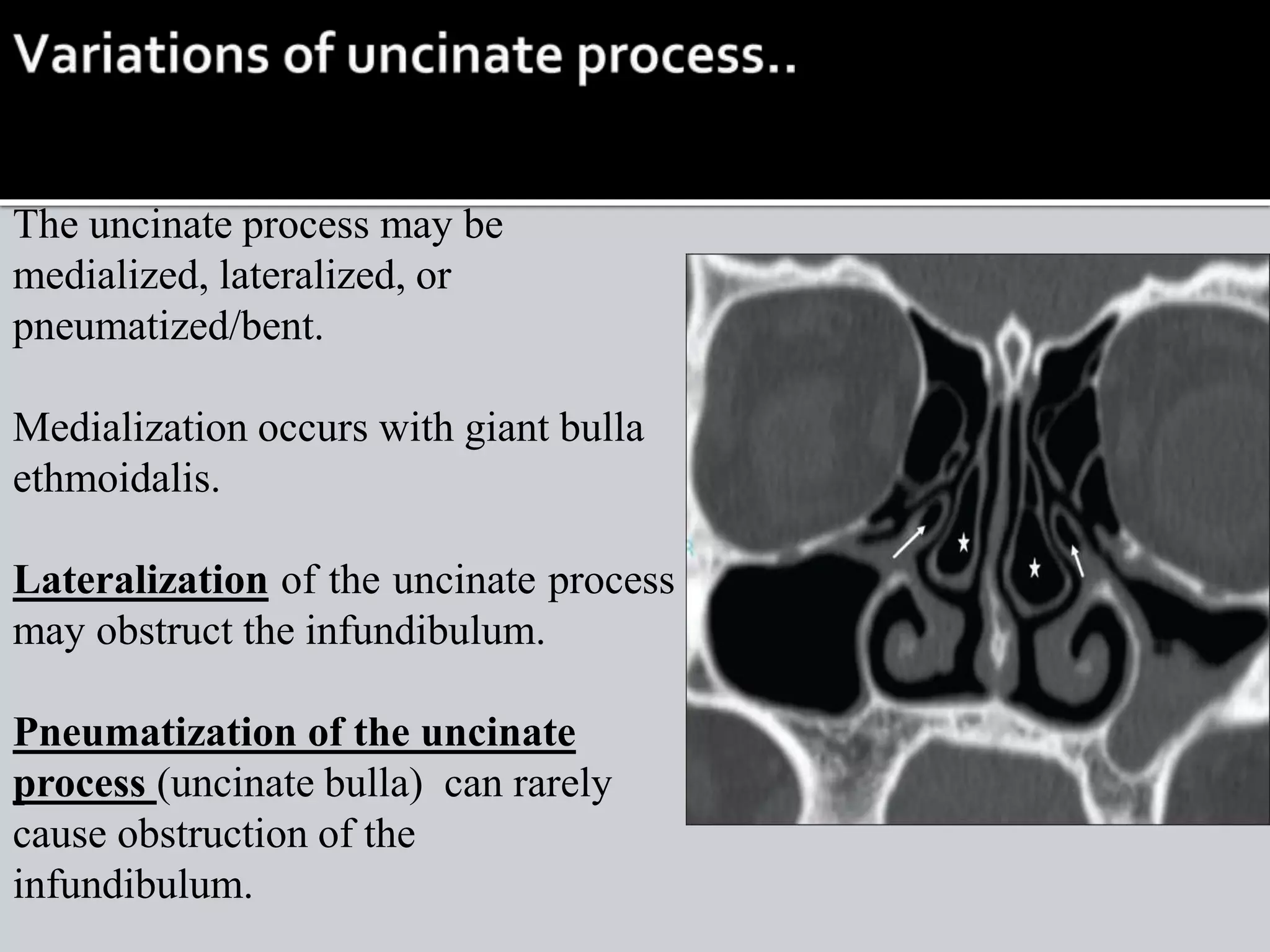

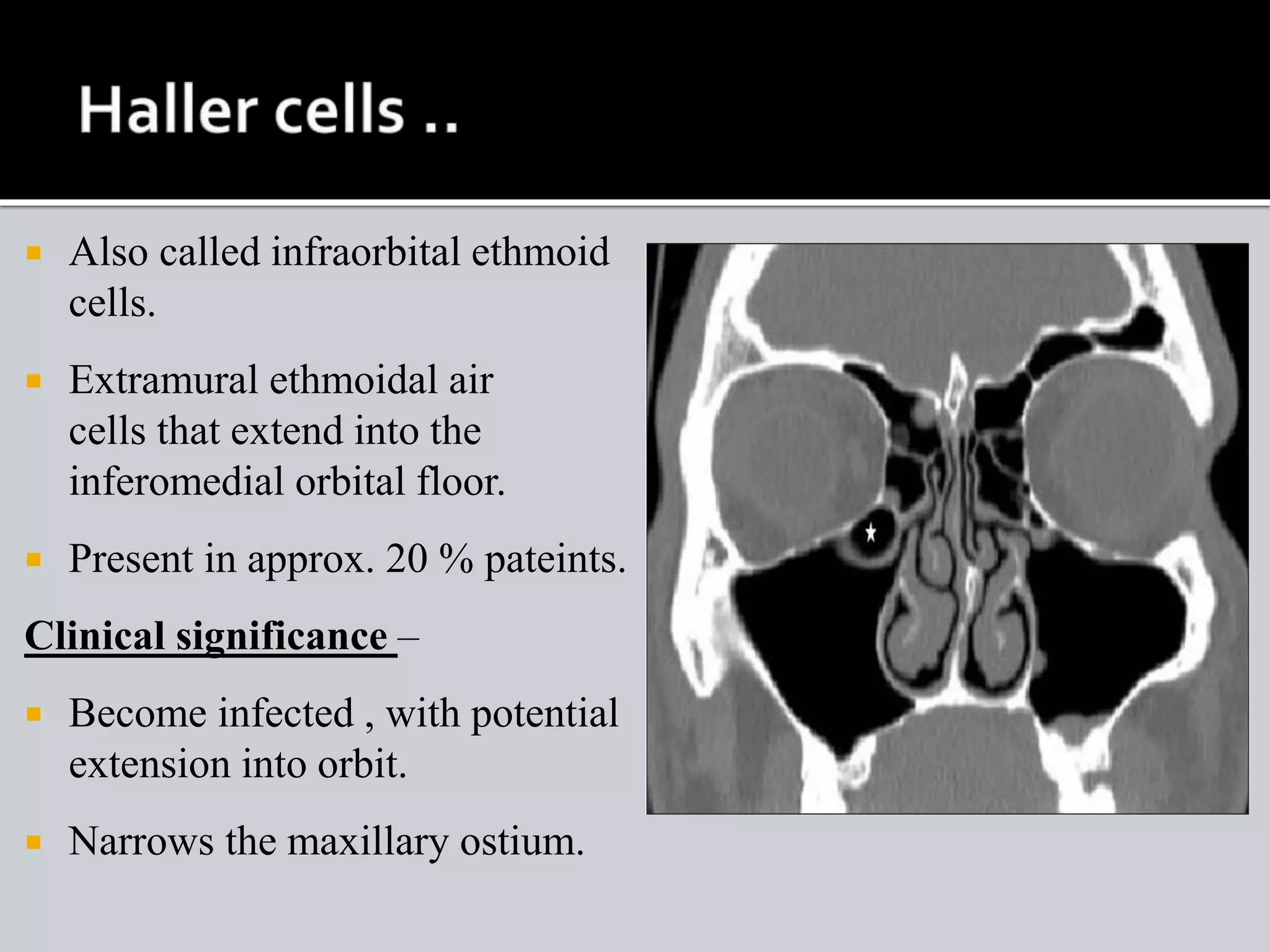













The document summarizes the anatomy and variations of the paranasal sinuses. It describes the locations and openings of the different sinus groups. Key anatomical structures involved in sinus drainage like the osteomeatal complex are also explained. Common anatomic variations seen on imaging that can affect sinus drainage are discussed. These variations include concha bullosa, Haller cells, Onodi cells and pneumatization of surrounding bones.












![Radiological anatomy of_temporal_bone[1]](https://cdn.slidesharecdn.com/ss_thumbnails/radiologicalanatomyoftemporalbone1-171112100915-thumbnail.jpg?width=640&height=640&fit=bounds)






























































