Downloaded 180 times




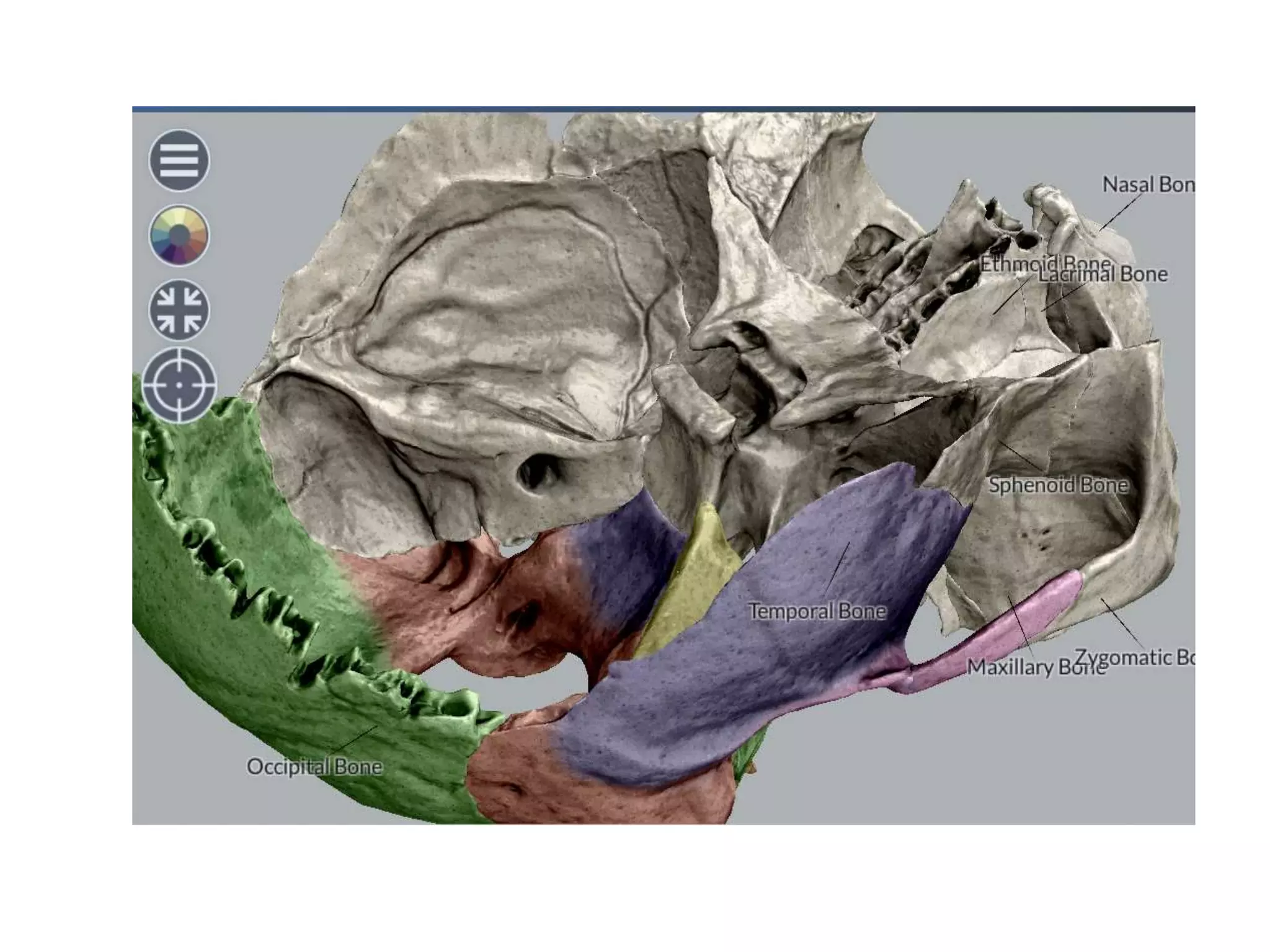







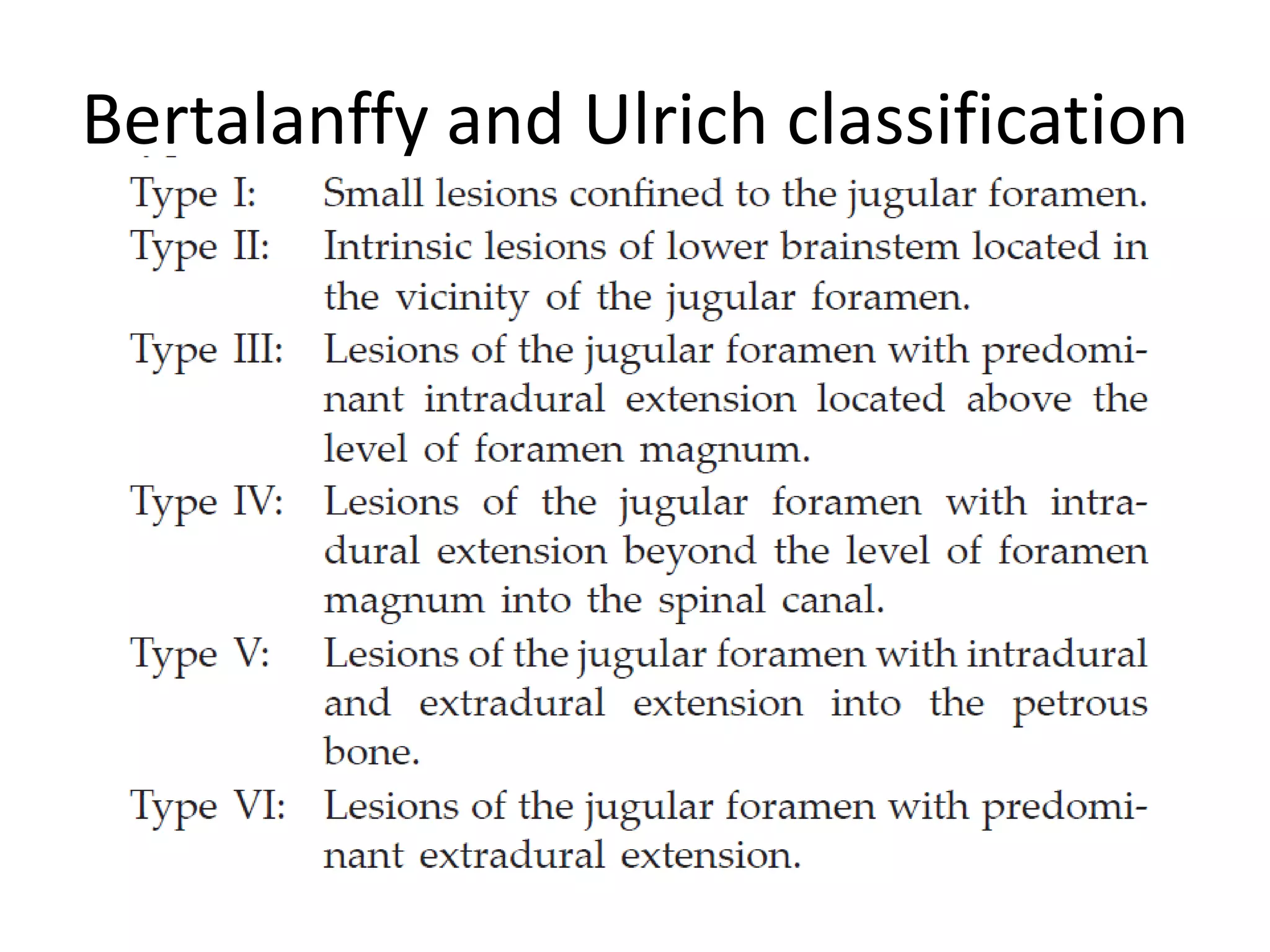











The jugular foramen is located at the skull base and formed by bones of the temporal and occipital bones. It contains nerves IX-XI and often the inferior petrosal sinus. Approaches to access the jugular foramen include posterior, lateral, and anterior. The posterior approach uses a suboccipital retrosigmoid, transcondylar, or supracondylar route. Lateral approaches are juxtacondylar or lateral skull base. Anterior approaches use a postauricular transtemporal or preauricular subtemporal route. Surgical techniques aim to expose the jugular foramen while preserving nearby structures like cranial nerves and vessels.