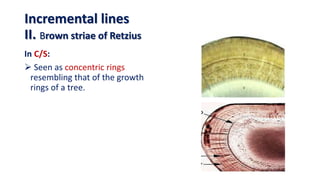
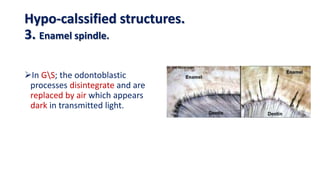
This document discusses the structure and properties of enamel. It begins by defining enamel as the outermost layer of tooth covering made of highly mineralized tissue. The structure of enamel is described including enamel rods, interrod substance, and rod sheaths. Physical properties like hardness, thickness and chemical composition consisting mainly of hydroxyapatite are covered. Incremental growth lines including cross striations, striae of Retzius and neonatal line are also summarized. Hypo-mineralized enamel structures such as enamel spindles, tufts and lamellae are defined. Finally, the surface structure of enamel including outer structureless enamel and perikymata grooves are described.